In the intricate world of healthcare, where patient care intersects with complex administrative systems, a series of alphanumeric characters holds immense power. For the patient suffering from debilitating abdominal cramps, urgent diarrhea, and fatigue, their condition has a name: colitis. For the gastroenterologist who diagnoses and treats them, it is a clinical challenge. But for the medical coder, the health information manager, and the healthcare system at large, that condition must be translated into a precise, universal language—the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). This translation is not a mere clerical task; it is a critical function that directly influences patient outcomes, drives medical research, and determines the financial viability of healthcare providers.
Colitis, simply defined as inflammation of the colon, is not a single disease but a umbrella term for a wide array of disorders with varying causes, severities, and treatments. A code for “colitis” is as nonspecific as a code for “arm pain”—it may be technically correct, but it fails to capture the essential details needed for effective care and accurate data analysis. Was the colitis triggered by a transient bacterial infection? Is it a chronic, lifelong autoimmune condition like ulcerative colitis? Did it develop as a side effect of radiation therapy for cancer? Or is it a life-threatening complication of C. difficile infection in a hospitalized patient?
This article serves as an exhaustive guide to navigating the complex landscape of ICD-10 codes for colitis. We will move beyond superficial code lists and delve into the pathophysiology of different colitis types, the logical structure of the ICD-10 system, and the nuanced decision-making process required for accurate coding. Our journey will equip medical coders, students, healthcare providers, and practice managers with the knowledge to ensure that every digit in a colitis code tells the true and complete story of the patient’s condition. By mastering this specificity, we contribute to a healthcare ecosystem that is more efficient, more knowledgeable, and ultimately, more humane.
ICD-10 Codes for Colitis
2. Understanding Colitis: A Primer on Inflammation of the Colon
Before a single code can be assigned, a fundamental understanding of the condition itself is paramount.
The Anatomy of the Colon
The colon, or large intestine, is the final segment of the digestive tract. It is a muscular tube approximately five feet long, responsible for absorbing water and electrolytes from indigestible food matter, forming and storing feces until elimination. Its lining, the mucosa, is a delicate layer of epithelial cells that is highly susceptible to inflammation. When this lining becomes inflamed—a condition known as colitis—its normal functions are disrupted, leading to the classic symptoms of diarrhea (as water absorption fails), abdominal pain, and often, rectal bleeding or pus.
The Spectrum of Colitis: From Acute to Chronic
Colitis manifests across a broad spectrum:
-
Acute Colitis: This has a sudden onset and is often short-lived. Common causes include bacterial or viral infections (Salmonella, C. difficile), ischemic injury (lack of blood flow), or a transient reaction to a toxin. Symptoms can be severe but typically resolve with treatment of the underlying cause.
-
Chronic Colitis: This type persists for weeks, months, or a lifetime, often with periods of flare-ups and remission. The prime examples are Inflammatory Bowel Disease (IBD), which includes Ulcerative Colitis (UC) and Crohn’s Disease. These are autoimmune conditions where the body’s immune system mistakenly attacks the colon. Microscopic colitis (lymphocytic and collagenous) is another form of chronic inflammation diagnosed via biopsy.
-
Indeterminate Colitis: In about 10-15% of cases, even after extensive testing, clinicians cannot definitively distinguish between ulcerative colitis and Crohn’s disease affecting the colon. This diagnostic uncertainty has a specific coding implication.
This pathophysiological diversity is the very reason the ICD-10-CM system requires such a high level of specificity. Coding “colitis” without an etiological specification is clinically inadequate.
3. The Foundation of Medical Coding: An Overview of the ICD-10-CM System
What is ICD-10-CM and Why Does It Matter?
The ICD-10-CM is the United States’ clinical modification of the World Health Organization’s (WHO) ICD-10, which is used for mortality statistics. ICD-10-CM is used for classifying diagnoses and reasons for visits in all healthcare settings. Its importance is multifaceted:
-
Standardization: It provides a common language for diseases, injuries, and health conditions.
-
Reimbursement: It is the foundation for billing and reimbursement. Incorrect codes can lead to claim denials, underpayments, or audits.
-
Epidemiology and Research: It allows for the tracking of disease prevalence, treatment outcomes, and public health trends.
-
Quality Measurement: It helps in assessing the quality of care and patient safety indicators.
The Structure of an ICD-10 Code: A Hierarchical Language
An ICD-10-CM code is not a random string. It is a hierarchical code that tells a story:
-
Chapter: The first character is a letter, representing the chapter. Most digestive system diseases, including colitis, fall under Chapter 11: Diseases of the Digestive System (K00-K95).
-
Category: The first three characters (e.g., K52) represent the category of the disease.
-
Subcategory and Extension: Characters after the decimal point provide greater specificity regarding etiology, anatomical site, severity, and other clinical details. For example, K52.2 specifies “Allergic and dietetic gastroenteritis and colitis.”
This structure allows coders to drill down from a general condition to a highly specific diagnosis.
4. Navigating the ICD-10-CM Chapter for Digestive System Diseases (Chapter 11: K00-K95)
Chapter 11 encompasses all disorders of the oral cavity, esophagus, stomach, intestines, liver, pancreas, and gallbladder. The most relevant blocks for colitis are:
-
K20-K31: Diseases of esophagus, stomach, and duodenum.
-
K35-K38: Diseases of appendix.
-
K40-K46: Hernias.
-
K50-K52: Noninfective enteritis and colitis. This is the core block for chronic and non-infectious inflammatory conditions.
-
K55-K64: Other diseases of intestines, including diverticular disease (K57) and irritable bowel syndrome (K58).
-
K65-K68: Diseases of peritoneum.
It is crucial to note that infectious colitis is not coded in Chapter 11. It is found in Chapter 1: Certain Infectious and Parasitic Diseases (A00-B99). This separation is a fundamental principle in ICD-10 coding.
5. Deconstructing the Core Colitis Codes: K50-K52
This section provides a detailed analysis of the codes used for non-infectious colitis.
Ulcerative Colitis (K50): A Deep Dive into a Chronic Condition
Ulcerative Colitis is characterized by continuous inflammation starting at the rectum and extending proximally to involve varying portions of the colon. The extent of involvement is critical for coding.
-
K50.0 – Ulcerative (chronic) pancolitis: This code is used when the entire colon is inflamed. This is often the most severe form.
-
K50.1 – Ulcerative (chronic) proctitis: Inflammation is confined to the rectum. This is often a milder form.
-
K50.8 – Other ulcerative colitis: This is a vital code for specifying the extent of disease when it is not pancolitis or proctitis. This includes:
-
Ulcerative proctosigmoiditis: Inflammation of the rectum and sigmoid colon.
-
Left-sided colitis: Inflammation extending from the rectum up to the splenic flexure.
-
-
K50.9 – Ulcerative colitis, unspecified: This code should be used only when the medical documentation does not specify the extent of the disease. It is a less desirable code and efforts should be made to obtain more specific documentation.
Coding Scenarios and Clinical Documentation Challenges:
A provider’s note that simply states “UC flare” is insufficient. The coder must look for clues in the endoscopy or histopathology report. Phrases like “inflammation to the hepatic flexure” or “severe proctosigmoiditis” guide the coder to K50.8. If no detail is available, K50.9 is assigned.
Crohn’s Disease [Regional Enteritis] (K50): When Colitis is Part of a Larger Picture
Crohn’s disease can affect any part of the gastrointestinal tract, from mouth to anus, but most commonly affects the end of the small intestine (ileum) and the beginning of the colon. Unlike UC, the inflammation is not continuous; it is “skip lesions” with healthy tissue in between.
-
K50.0 – Crohn’s disease of small intestine: Used when the disease is confined to the small bowel.
-
K50.1 – Crohn’s disease of large intestine: This is “Crohn’s colitis.” Used when the disease is confined to the colon.
-
K50.8 – Other Crohn’s disease: This code is for cases where the disease affects both the small and large intestine (ileocolitis), or other specified sites like the stomach or mouth.
-
K50.9 – Crohn’s disease, unspecified: Used when the site is not documented.
Other and Unspecified Noninfective Gastroenteritis and Colitis (K52): The Catch-All Category
This category is a collection of various types of colitis that are not infectious, UC, or Crohn’s. It is a highly important and often-used category.
-
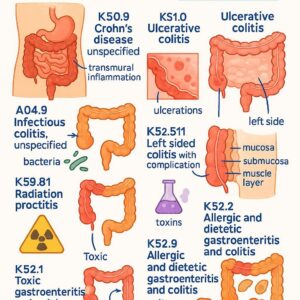
K52.0 – Gastroenteritis and colitis due to radiation: A common side effect of radiation therapy for abdominal or pelvic cancers (e.g., prostate, cervical cancer).
-
K52.1 – Toxic gastroenteritis and colitis: This refers to inflammation caused by a toxic agent. Note: This does not refer to toxic megacolon (which is coded as K59.3, a complication). This is for conditions like food poisoning from bacterial toxins.
-
K52.2 – Allergic and dietetic gastroenteritis and colitis: This includes food-protein-induced enterocolitis syndrome (FPIES) and other allergic reactions affecting the colon.
-
K52.3 – Indeterminate colitis: As discussed earlier, this is used when a definitive diagnosis of UC or Crohn’s cannot be made after pathological examination of a colectomy specimen.
-
K52.8 – Other specified noninfective gastroenteritis and colitis: This is a broad category that includes:
-
Microscopic Colitis: This includes both lymphocytic colitis and collagenous colitis. These are diagnosed by biopsy and are characterized by chronic watery diarrhea without visible inflammation on colonoscopy. Coding Note: There is no specific code for microscopic colitis, so K52.8 is the appropriate choice.
-
Eosinophilic colitis
-
-
K52.9 – Noninfective gastroenteritis and colitis, unspecified: This is the least specific code and should be a last resort. It is for cases of “colitis” or “gastroenteritis” where no cause (infectious or otherwise) is identified or documented. It is often incorrectly used when a more specific code is available.
Summary of Key Non-Infectious Colitis Codes (K50-K52)
| ICD-10 Code | Code Description | Clinical Example | Documentation Key Words |
|---|---|---|---|
| K50.0 | Ulcerative pancolitis | Inflammation of the entire colon on colonoscopy. | “Pancolitis”, “total colitis”, “inflammation extending to the cecum” |
| K50.1 | Ulcerative proctitis | Inflammation limited to the rectum. | “Proctitis”, “inflammation confined to the rectum” |
| K50.8 | Other ulcerative colitis | Inflammation of the left colon. | “Proctosigmoiditis”, “left-sided colitis”, “distal colitis” |
| K50.9 | Ulcerative colitis, unspecified | Note only states “UC flare” without location. | “Ulcerative colitis” (without further specification) |
| K50.10 | Crohn’s disease of large intestine | Inflammation of the colon with skip lesions. | “Crohn’s colitis”, “granulomatous colitis” |
| K50.11 | Crohn’s disease of small intestine | Terminal ileitis. | “Ileal Crohn’s”, “small bowel Crohn’s” |
| K52.0 | Radiation colitis | Diarrhea and bleeding after pelvic radiation. | “Radiation proctitis/colitis”, “actinic colitis” |
| K52.2 | Allergic colitis | Infant with bloody stools due to cow’s milk protein allergy. | “Allergic proctocolitis”, “food protein-induced” |
| K52.3 | Indeterminate colitis | Pathology report states “indeterminate colitis” after surgery. | “Indeterminate colitis” |
| K52.8 | Other specified noninfective | Diagnosis of lymphocytic colitis on biopsy. | “Microscopic colitis”, “lymphocytic colitis”, “collagenous colitis” |
| K52.9 | Noninfective gastroenteritis and colitis, unspecified | Patient with diarrhea, no infectious cause found, no other diagnosis given. | “Colitis”, “gastroenteritis” (non-specific) |
6. Infectious Agents as the Culprit: Coding for Infectious Colitis (A00-A09)
When colitis is caused by a pathogen, coding shifts to Chapter 1. The code selection depends entirely on the specific organism identified.
-
A04.7 – Enterocolitis due to Clostridium difficile: This is one of the most important codes for hospital coders. C. diff colitis is a major healthcare-associated infection, often occurring after antibiotic use. POA Indicator: The Present-on-Admission (POA) indicator is critical here to determine if the infection was acquired during the hospitalization.
-
A02.0 – Salmonella enteritis: For Salmonella infections.
-
A03.0 – Shigellosis due to Shigella dysenteriae: For Shigella infections.
-
A04.0 – Enteropathogenic Escherichia coli infection: For specific pathogenic E. coli strains.
-
A08.0 – Rotaviral enteritis: Common in children.
-
A09 – Infectious gastroenteritis and colitis, unspecified: This is the equivalent of K52.9 for infectious cases. It should be used only when a provider documents “infectious gastroenteritis” or “infectious colitis” but does not specify the organism.
Coding Rule: If a specific organism is documented, you must use the specific code (e.g., A04.7 for C. diff), not the unspecified A09 code.
7. Specificity is Key: Documenting and Coding for Manifestations and Complications
Colitis is often accompanied by complications or manifestations that are critical to the patient’s condition. ICD-10-CM guidelines provide instructions for coding these.
-
Hemorrhage (R58.-): If the colitis is actively bleeding, code R58 (Hemorrhage, not elsewhere classified) may be reported as an additional diagnosis. However, always check the Alphabetic Index. For “Colitis, hemorrhagic,” it directs you to the underlying colitis code (e.g., K52.9), as hemorrhage is a common symptom. The additional code may be needed if the bleeding is severe and a specific focus of treatment.
-
Dehydration (E86.0): Many forms of colitis cause severe diarrhea, leading to dehydration. Code E86.0 is always added as a secondary diagnosis when documented.
-
Megacolon (K59.3): Toxic megacolon is a life-threatening complication where the colon dilates and can rupture. It is a medical emergency. It is coded separately as K59.3 (Megacolon, not elsewhere classified). The underlying cause (e.g., A04.7 for C. diff, K50.0 for UC) is sequenced first, followed by K59.3.
-
Fistulas and Abscesses in Crohn’s Disease: These are common complications of Crohn’s. They have their own codes (e.g., K50.314 for a fistula, K50.014 for an abscess) and are integral to the disease process. The coding guidelines provide specific instructions for sequencing.
8. The Art of Sequencing: Primary Diagnosis, Comorbidities, and Present-on-Admission (POA)
Sequencing—the order in which codes are listed—is crucial. The first-listed diagnosis (outpatient) or principal diagnosis (inpatient) is the condition chiefly responsible for the encounter.
-
Inpatient Example: A patient is admitted for a severe flare of Crohn’s colitis. The principal diagnosis is K50.11 (Crohn’s disease of large intestine). If they are also dehydrated, E86.0 (Dehydration) is listed as a secondary diagnosis.
-
POA Indicator: For inpatient claims, each diagnosis must be marked as Present-on-Admission (Y) or Not (N). A C. diff infection that develops after the third hospital day would be marked “N,” which has implications for hospital reimbursement (as it may be considered a hospital-acquired condition).
9. Case Studies: Applying ICD-10 Codes to Real-World Patient Encounters
Case Study 1: The Flare-Up
-
Scenario: A 35-year-old female with a known history of ulcerative pancolitis presents to her gastroenterologist for a scheduled follow-up. She reports a two-week history of increased bowel frequency (8-10 times/day) with blood and mucus, along with significant fatigue. The physician’s note states: “Patient experiencing a flare of her known ulcerative pancolitis. Current symptoms consistent with active disease.”
-
Coding: K50.0 (Ulcerative pancolitis). The reason for the encounter is the management of the underlying chronic condition. The “flare” is not a separate code; it is the manifestation of the active disease.
Case Study 2: The Hospitalized Patient
-
Scenario: An 80-year-old male was admitted for pneumonia treated with intravenous antibiotics. On hospital day 5, he develops profuse, watery diarrhea and abdominal pain. A C. difficile PCR test returns positive. The physician diagnoses “Healthcare-associated Clostridium difficile colitis.”
-
Coding:
-
Principal Diagnosis: The reason for the original admission was pneumonia (J18.9). However, the development of C. diff colitis extends the stay and becomes the focus of major treatment. After careful review of the UHDDS guidelines, the C. diff may be sequenced as principal if it meets the definition. Often, the original condition remains principal. This requires clinical judgment.
-
Codes:
-
J18.9 (Pneumonia, unspecified organism) – Principal Diagnosis (if the pneumonia is still being treated).
-
A04.72 (Enterocolitis due to Clostridium difficile, hospital-acquired) – Secondary Diagnosis. POA = N (Not Present on Admission).
-
-
*Alternatively, if the pneumonia is resolved and the entire focus is on treating the life-threatening colitis, A04.72 could be sequenced as principal.*
-
Case Study 3: The New Diagnosis
-
Scenario: A 22-year-old male is admitted with a two-month history of crampy abdominal pain, weight loss, and bloody diarrhea. A colonoscopy is performed with biopsies. The pathology report concludes: “Active chronic colitis. Features are not definitive for either ulcerative colitis or Crohn’s disease. Best classified as indeterminate colitis.”
-
Coding: K52.3 (Indeterminate colitis). This is the specific code for this exact pathological diagnosis.
10. The Impact of Accurate Colitis Coding: Beyond the Medical Record
The ripple effects of precise coding extend far beyond the patient’s chart:
-
Reimbursement: A code for unspecified colitis (K52.9) may reimburse at a lower rate than a code for C. diff colitis (A04.7) or Crohn’s colitis (K50.11), which reflect higher complexity and resource use.
-
Research: Accurate data allows researchers to identify patient populations for clinical trials, track the effectiveness of new IBD drugs, and understand the long-term outcomes of different colitis types.
-
Public Health: Tracking codes for infectious colitis (A04.7, A02.0, etc.) is essential for detecting outbreaks in the community or in healthcare facilities.
11. Common Pitfalls and How to Avoid Them: A Coder’s Checklist
-
Pitfall: Assuming all colitis is coded in Chapter 11 (K00-K95).
-
Solution: Always ask, “Is it infectious?” If yes, go to Chapter 1 (A00-B99).
-
-
Pitfall: Using K52.9 (unspecified) when a more specific code is available in the documentation.
-
Solution: Scour the record for clues: endoscopy reports, pathology reports, and discharge summaries often contain the specific terminology needed.
-
-
Pitfall: Confusing “toxic colitis” (K52.1) with “toxic megacolon” (K59.3).
-
Solution: K52.1 refers to inflammation from a toxin. K59.3 is a specific, severe complication characterized by colon dilation.
-
-
Pitfall: Not adding codes for important complications like dehydration (E86.0) or megacolon (K59.3).
-
Solution: Review the entire record for documented manifestations that affect patient care.
-
12. Looking Ahead: The Future of Colitis Classification and ICD-11
The World Health Organization has already released ICD-11. While the US has not yet set a transition date, it’s important to be aware of future changes. ICD-11 offers even greater granularity and a more modern, digital-friendly structure. For example, it has specific entity codes for “Lymphocytic colitis” and “Collagenous colitis” (DA96.4), eliminating the need for the “other specified” code (K52.8) currently used in ICD-10-CM.
13. Conclusion: Mastering the Nuances for Optimal Patient Care and Data Integrity
Accurate ICD-10 coding for colitis is a demanding but essential discipline that bridges clinical care and health information science. It requires a deep understanding of gastrointestinal pathology, a meticulous approach to reading medical documentation, and a firm grasp of the ICD-10-CM guidelines. By moving beyond generic terms and embracing the specificity that the coding system offers—distinguishing between ulcerative pancolitis and infectious C. diff colitis, or between Crohn’s disease and microscopic colitis—we ensure that the data generated truly reflects the patient’s experience. This precision fuels everything from correct reimbursement and advanced clinical research to effective public health monitoring, ultimately contributing to a higher standard of care for all patients suffering from these complex and challenging conditions.
14. Frequently Asked Questions (FAQs)
Q1: What is the difference between ICD-10 code K52.9 and A09?
A: K52.9, “Noninfective gastroenteritis and colitis, unspecified,” is used when the cause is unknown or not specified, but an infectious cause is ruled out or not suspected. A09, “Infectious gastroenteritis and colitis, unspecified,” is used when the provider documents an infectious cause but does not identify the specific organism. The key differentiator is the provider’s documentation regarding the suspected etiology.
Q2: How do I code microscopic colitis (lymphocytic or collagenous colitis)?
A: In ICD-10-CM, there is no unique code for microscopic colitis. The appropriate code is K52.8 (Other specified noninfective gastroenteritis and colitis). It is crucial to ensure the documentation explicitly states “lymphocytic colitis” or “collagenous colitis” to justify using this more specific code over K52.9.
Q3: A patient has ulcerative colitis and is admitted for a C. difficile infection. What is the principal diagnosis?
A: This is a classic sequencing dilemma. The decision is based on the circumstances of admission. If the patient was admitted because the C. diff infection caused a severe deterioration, then A04.7 (Enterocolitis due to C. difficile) would be the principal diagnosis, with K50.- (Ulcerative colitis) listed as a secondary/comorbid condition. If the patient was admitted for an UC flare and acquired C. diff in the hospital, the UC would likely remain principal. The coder must apply the UHDDS guidelines and, if uncertain, query the provider.
Q4: When should I use an additional code for dehydration (E86.0) with colitis?
A: Code E86.0 should be assigned as a secondary diagnosis anytime dehydration is documented by the provider as a current clinical concern and is being monitored or treated. Severe diarrhea from colitis is a common cause of dehydration, and coding it reflects the complexity of the patient’s condition.
15. Additional Resources
-
CDC ICD-10-CM Official Guidelines for Coding and Reporting: https://www.cdc.gov/nchs/icd/icd-10-cm.htm (The definitive source for coding rules).
-
American Health Information Management Association (AHIMA): https://www.ahima.org/ (Provides educational resources and professional guidance for coders).
-
American Academy of Professional Coders (AAPC): https://www.aapc.com/ (Another leading organization for coder education and certification).
-
Crohn’s & Colitis Foundation: https://www.crohnscolitisfoundation.org/ (A valuable resource for understanding the clinical aspects of IBD).





