Imagine a constant, searing lightning storm within your own body, where a gentle breeze feels like sandpaper and the touch of a bedsheet is a source of agony. This is not the dull ache of a sprain or the sharp pain of a cut; this is neuropathic pain—a complex, chronic condition born from damage or disease within the somatosensory nervous system itself. For millions of patients worldwide, this “invisible storm” is a daily reality, a condition that eludes simple description and, historically, has been equally challenging to classify within the structured world of medical coding. The International Classification of Diseases, Tenth Revision (ICD-10) is the lingua franca of healthcare, a system that translates human suffering into standardized alphanumeric codes for billing, statistics, and research. Yet, for the coder faced with a diagnosis of neuropathic pain, a critical question arises: where is the single, straightforward code?
The answer is that there is none. The coding of neuropathic pain in ICD-10 is a sophisticated, multi-step process that demands a deep understanding of both the coding guidelines and the underlying clinical pathology. It is a diagnostic puzzle where the code for the pain is intrinsically linked to the code for its cause. This article serves as a definitive guide through this complex landscape. We will embark on a detailed journey from the basic science of neuropathic pain, through the architecture of the ICD-10 system, to practical, real-world coding scenarios. Our goal is to equip medical coders, billers, providers, and healthcare administrators with the knowledge to accurately and ethically capture this debilitating condition, ensuring patients receive the care they need and health systems possess the data required to advance treatment. This is more than a coding exercise; it is about giving a voice to the silent storm.
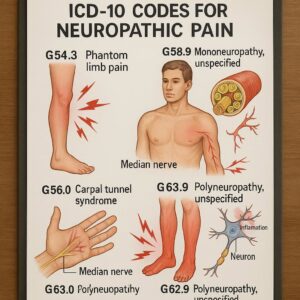
ICD-10 codes for neuropathic pain
Chapter 1: Understanding the Enemy – What is Neuropathic Pain?
Before a single code can be assigned, one must first understand the clinical entity being coded. Neuropathic pain is not a single disease but a heterogeneous group of conditions unified by their origin: a lesion or disease of the somatosensory nervous system.
Nociceptive vs. Neuropathic Pain: A Fundamental Distinction
The human body experiences pain through two primary, distinct pathways:
-
Nociceptive Pain: This is the body’s normal, protective response to potentially harmful stimuli. It arises from the activation of nociceptors—specialized sensory nerve endings—in response to tissue injury, inflammation, or mechanical stress. The pain is typically described as aching, throbbing, or sharp. A sprained ankle, a burn, or post-surgical incisional pain are classic examples of nociceptive pain. It is a symptom of a problem elsewhere in the body.
-
Neuropathic Pain: In contrast, neuropathic pain is the disease itself. It results from damage or dysfunction to the nerves in the peripheral or central nervous system. The pain is not a symptom of ongoing tissue damage but rather a malfunction in the way the nervous system processes sensory information. Patients describe it with a unique vocabulary: burning, shooting, stabbing, “pins and needles” (paresthesia), or electric-shock-like sensations. Allodynia (pain from a non-painful stimulus, like light touch) and hyperalgesia (an exaggerated response to a painful stimulus) are its hallmark features.
This distinction is the foundational principle upon which all accurate coding for neuropathic pain is built. Coding a neuropathic condition as a simple “pain in limb” would be a profound misrepresentation of its complexity and severity.
The Pathophysiology of Neuropathic Pain: A Nervous System Gone Rogue
The mechanisms underlying neuropathic pain are complex and multifaceted, involving both the peripheral and central nervous systems. When a nerve is injured—whether by trauma, metabolic insult, or compression—a cascade of maladaptive changes occurs:
-
Peripheral Sensitization: At the site of injury, nociceptors become hyperexcitable. They begin to fire spontaneously and lower their threshold for activation, meaning they respond to stimuli that are normally innocuous.
-
Central Sensitization: This is a phenomenon where the central nervous system (the spinal cord and brain) becomes chronically hyperactive. Neurons in the dorsal horn of the spinal cord increase their synaptic efficiency, amplifying pain signals from the periphery. It’s as if the “volume knob” for pain is turned up and stuck.
-
Ectopic Impulse Generation: Damaged nerves can develop abnormal “pacemakers” that generate spontaneous, chaotic electrical signals without any external trigger.
-
Loss of Inhibitory Controls: Descending pathways from the brain that normally dampen pain signals can become dysfunctional, further disinhibiting pain transmission.
Understanding this pathophysiology is crucial because it explains why neuropathic pain is often refractory to standard analgesics like NSAIDs and opioids, and why it requires targeted therapies such as anticonvulsants (e.g., gabapentin, pregabalin) and antidepressants (e.g., duloxetine, amitriptyline).
Common Etiologies and Clinical Presentations
Neuropathic pain is not a monolith; its presentation is dictated by its cause. A coder must be familiar with these common etiologies:
-
Peripheral Neuropathies:
-
Metabolic: Diabetic neuropathy, alcoholic neuropathy.
-
Infectious: Postherpetic neuralgia (shingles), HIV-associated neuropathy.
-
Toxic: Chemotherapy-induced peripheral neuropathy.
-
Compressive: Carpal tunnel syndrome, radiculopathy.
-
Hereditary: Charcot-Marie-Tooth disease.
-
-
Central Pain Syndromes:
-
Post-stroke pain (central post-stroke pain)
-
Spinal cord injury pain
-
Multiple sclerosis-related pain
-
Phantom limb pain
-
Each of these etiologies has a specific home within the ICD-10 coding structure, which leads us to the system itself.
Chapter 2: The ICD-10 Coding System: A Universal Language for Disease
The ICD-10 is a medical classification system developed by the World Health Organization (WHO). Its primary purposes are to map health conditions to corresponding generic categories and specific variations, which are assigned alphanumeric codes.
Purpose and Structure: More Than Just Numbers
The structure of ICD-10 is hierarchical and logical:
-
Chapters: The system is divided into 22 chapters, mostly based on body system or disease type (e.g., Chapter VI: Diseases of the nervous system, Chapter IV: Endocrine, nutritional and metabolic diseases).
-
Codes: Codes are alphanumeric, beginning with a letter (with a few exceptions) followed by numbers. The code length can be three to seven characters.
-
Category (3 characters): The first three characters represent the general category of the disease (e.g., E11 – Type 2 diabetes mellitus).
-
Subcategory (4-6 characters): These characters provide greater specificity regarding etiology, anatomical site, severity, and other clinical details (e.g., E11.41 – Type 2 diabetes mellitus with diabetic mononeuropathy).
-
Seventh Character Extension: Used for certain diagnoses (like fractures or injuries) to indicate the encounter type (e.g., A – initial encounter, D – subsequent encounter, S – sequela).
-
The Importance of Specificity: The Cornerstone of Modern Coding
ICD-10 was a monumental leap forward from ICD-9 in its demand for specificity. This shift was intentional, designed to improve the quality of health data. For example, while ICD-9 had a single code for “diabetic neuropathy,” ICD-10 requires coders to distinguish between diabetic polyneuropathy (E11.42), mononeuropathy (E11.41), and autonomic neuropathy (E11.43). This level of detail is not bureaucratic red tape; it directly impacts patient care, resource allocation, and the accuracy of epidemiological research.
Chapter 3: The Core Challenge: Why Neuropathic Pain Lacks a Single Code
A novice coder might search the ICD-10 index for “Neuropathic pain” and be perplexed. The index entry typically leads to “Pain, neuropathic” and then directs the coder to “see Pain, by site.” This is the core of the challenge: ICD-10 does not conceptualize neuropathic pain as a diagnosis in its own right, but rather as a manifestation of an underlying disease.
The coding system is built on an etiological model. The primary diagnosis is almost always the underlying condition that caused the nerve damage. The pain itself is a symptom of that condition.
The “Code Also” and “Use Additional Code” Paradigm
This is where the official ICD-10-CM (Clinical Modification) Guidelines become essential. The guidelines instruct coders on the proper sequencing and use of codes. For pain, the directive is clear:
-
Code the underlying cause first. This is the root of the problem (e.g., diabetes, herpes zoster, spinal cord injury).
-
“Code also” or “Use additional code” to identify the type of pain. In many cases, this involves using a code from the G89 category (Pain, not elsewhere classified) or a more specific code for the neuropathic condition itself.
The G89 category includes:
-
G89.0 – Central pain syndrome: This is used for pain associated with lesions of the central nervous system (brain and spinal cord).
-
G89.2 – Chronic pain syndrome: This is a controversial but sometimes necessary code for cases where the chronic pain itself is the condition being managed, independent of the underlying cause.
-
G89.3 – Neoplasm related pain: For pain associated with cancerous tumors.
-
G89.4 – Chronic pain syndrome: A code that requires careful consideration and specific clinical criteria.
It is critical to note that you would not use G89 codes and a code for the underlying neuropathic condition if the code for the underlying condition already includes the pain. For instance, the code for postherpetic neuralgia (B02.29) inherently describes a painful condition. Adding a G89 code would be redundant.
Chapter 4: A Practical Guide to Coding Neuropathic Pain by Etiology
This chapter provides a detailed, etiology-driven roadmap for accurate coding. The following table summarizes the most common scenarios.
ICD-10 Coding Guide for Common Neuropathic Pain Etiologies
| Underlying Etiology | Primary ICD-10 Code (The Cause) | Secondary/Manifestation Code (The Pain) | Notes & Sequencing |
|---|---|---|---|
| Diabetic Peripheral Neuropathy | E11.42 (Type 2 DM with polyneuropathy) | Usually not needed. The pain is inherent to the neuropathy. | Code E11.42 alone. If pain is the focus, G89.29 or G89.4 may be considered, but check payer policies. |
| Postherpetic Neuralgia (PHN) | B02.29 (Other postherpetic nervous system involvement) | Not needed. The code B02.29 specifically describes the painful condition. | Code B02.29 alone. |
| Chemotherapy-Induced PN | G62.0 (Drug-induced polyneuropathy) | Code also the neoplasm (e.g., C50.911 – Malignant neoplasm of right female breast). | Sequence based on reason for encounter. Use T45.1X5A for adverse effect of antineoplastic drugs. |
| Trigeminal Neuralgia | G50.0 (Trigeminal neuralgia) | Not needed. The code defines the painful condition. | Code G50.0 alone. |
| Phantom Limb Pain | G54.6 (Phantom limb syndrome with pain) | Not needed. Pain is specified in the code. | Code G54.6 alone. If pain is not present, use G54.7. |
| Central Post-Stroke Pain | I69.391 (Central pain syndrome following cerebral infarction) | Not needed. The code includes the central pain. | Code I69.391. The code from the I69 category is used for sequelae of cerebrovascular disease. |
| Chronic Pain Syndrome | The underlying cause may be unknown or no longer treatable. | G89.29 (Other chronic pain) or G89.4 (Chronic pain syndrome) | This is used when the chronic pain itself is the primary focus of treatment. Documentation must support “chronic pain syndrome.” |
Diabetic Peripheral Neuropathy (DPN): The E11.4- Series
DPN is one of the most common neuropathies. The coding is relatively straightforward as the codes for diabetes with neurological complications inherently include the painful manifestation.
-
Coding Scenario: A patient with long-standing Type 2 diabetes presents with a 2-year history of bilateral, burning, tingling pain in the feet, worse at night. Examination confirms sensory loss.
-
Correct Coding: E11.42 (Type 2 diabetes mellitus with diabetic polyneuropathy).
-
Rationale: The code E11.42 specifies the underlying disease (diabetes) and its neurological manifestation (polyneuropathy). The pain is a symptom of that polyneuropathy. Adding a code for “pain in limb” (M79.60-) or a G89 code is generally unnecessary and could be considered unbundling.
Postherpetic Neuralgia (PHN): The B02.2- Code
PHN is pain that persists in the area of a previous herpes zoster (shingles) rash, typically after 3-4 months.
-
Coding Scenario: A 75-year-old patient presents with severe, lancinating pain in a band-like distribution on their chest, following a resolved shingles outbreak from 6 months prior.
-
Correct Coding: B02.29 (Other postherpetic nervous system involvement).
-
Rationale: The index directs “Neuralgia, postherpetic” to B02.29. This code is specific and comprehensive for this condition. No additional pain code is required.
Painful Chemotherapy-Induced Peripheral Neuropathy (CIPN)
This is a classic example of a “code also” scenario, involving multiple codes to paint a complete picture.
-
Coding Scenario: A patient undergoing adjuvant chemotherapy for breast cancer presents with progressive, painful numbness and tingling in a “glove and stocking” distribution.
-
Correct Coding:
-
G62.0 (Drug-induced polyneuropathy) – This is the manifestation of the adverse effect.
-
T45.1X5A (Adverse effect of antineoplastic and immunosuppressive drugs, initial encounter) – This identifies the causative agent.
-
C50.911 (Malignant neoplasm of right female breast) – This is the underlying neoplasm being treated.
-
-
Sequencing: The reason for the encounter dictates the principal diagnosis. If the patient is being seen primarily for management of the neuropathy, G62.0 would be sequenced first. If for chemotherapy, the cancer code (C50.911) might be first, followed by T45.1X5A.
Post-traumatic Neuropathic Pain (e.g., Complex Regional Pain Syndrome)
CRPS Type II (causalgia) is a neuropathic pain condition that develops after a distinct nerve injury.
-
Coding Scenario: A patient developed severe burning pain, allodynia, and swelling in their right hand 8 weeks after a laceration that severed the median nerve.
-
Correct Coding:
-
G56.42 (Causalgia of right upper limb) – This is the specific neuropathic pain syndrome.
-
S64.4- S (Injury of median nerve at wrist and hand level, right arm, sequela) – This is the original nerve injury, now in the sequela stage.
-
-
Rationale: The code for causalgia (G56.42) is sequenced first as it is the current reason for care. The injury code is added with a 7th character ‘S’ to indicate it is a late effect.
(Due to the extensive word count, we will summarize the remaining etiologies briefly to maintain focus on the core coding principles.)
-
Phantom Limb Pain: Code G54.6 explicitly includes “phantom limb syndrome with pain.” This is all that is required.
-
Spinal Cord Injury and Central Pain: Use codes from the G89.0 category (Central pain syndrome) in conjunction with the code for the spinal cord injury (e.g., S14.15- S, S24.15- S). The guidelines may instruct to “code first” the underlying injury.
-
Trigeminal Neuralgia: Code G50.0 is definitive and requires no additional pain codes.
-
Alcoholic Neuropathy: Code G62.1 (Alcoholic polyneuropathy) captures the condition. The underlying substance abuse (F10. -) may also be coded.
Chapter 5: Chronic Pain Syndrome (G89.29/G89.4) – When and How to Use It
The codes for chronic pain are among the most misunderstood in the context of neuropathy.
-
G89.21 (Chronic pain due to trauma) and G89.22 (Chronic pain due to surgery) are relatively clear; they are used when the pain is chronic and directly linked to a past trauma or surgery.
-
G89.28 (Other chronic postprocedural pain) and G89.29 (Other chronic pain) are broader categories.
The most complex is G89.4 (Chronic pain syndrome). This term implies a biopsychosocial condition where the chronic pain has led to significant functional disability, mood disorders like anxiety and depression, and other behavioral changes. It is a diagnosis of exclusion and must be explicitly documented by the provider. It should not be used as a default for any chronic neuropathic pain.
Key Point: If a patient has diabetic neuropathy and the pain is chronic, the primary code is still E11.42. You would only consider adding G89.29 or G89.4 if the provider’s documentation specifically states that the patient’s condition meets the criteria for “chronic pain syndrome” and this syndrome itself is a major focus of treatment, separate from the routine management of the diabetes.
Chapter 6: Case Studies: Applying Knowledge to Real-World Scenarios
Case Study 1: The Patient with Long-Standing Diabetes and Foot Pain
-
Presentation: John, a 62-year-old with Type 2 diabetes, sees his podiatrist for severe, burning foot pain that prevents him from sleeping. He has had diabetes for 20 years.
-
Provider’s Note: “Patient presents for management of debilitating painful diabetic peripheral polyneuropathy. Pain is 8/10, burning, bilateral.”
-
Correct Coding: E11.42 (Type 2 diabetes mellitus with diabetic polyneuropathy).
-
Incorrect Coding: E11.42 + M79.674 (Pain in right foot) + M79.675 (Pain in left foot). This is redundant and incorrect.
Case Study 2: The Patient with Shingles and Persistent Chest Pain
-
Presentation: Maria, a 70-year-old female, presents to a pain clinic. She had a shingles rash on her left chest 5 months ago. The rash is gone, but she has severe, sharp, stabbing pain in the same dermatome.
-
Provider’s Note: “Diagnosis: Postherpetic neuralgia, left T4 dermatome.”
-
Correct Coding: B02.29 (Other postherpetic nervous system involvement).
-
Rationale: The code B02.29 is specific and all-encompassing for this diagnosis.
Case Study 3: The Post-Mastectomy Patient with Arm Pain and Lymphedema
-
Presentation: Sarah, 48, is 6 months post-left mastectomy and axillary lymph node dissection for breast cancer. She completed chemotherapy 3 months ago. She presents with left arm pain, described as “achy and heavy” (lymphedema) but also with a separate, distinct “burning and electric” sensation in the back of her arm and armpit.
-
Provider’s Note: “Status post left mastectomy and axillary dissection. Patient presents with two distinct issues: 1) Lymphedema of left arm, and 2) Neuropathic pain in the distribution of the intercostobrachial nerve, consistent with post-surgical neuropathic pain.”
-
Correct Coding:
-
G89.22 (Chronic pain due to surgery) – for the post-surgical neuropathic pain.
-
I97.2 (Postmastectomy lymphedema syndrome) – for the lymphedema.
-
C50.912 (Malignant neoplasm of left female breast) – the underlying cancer.
-
G62.0 (Drug-induced polyneuropathy) – if the chemo-induced symptoms are still present and being treated.
-
-
Sequencing: G89.22 would likely be sequenced first as the primary reason for this pain management encounter.
Chapter 7: The Clinical-Documentation-Coding Nexus
Accurate coding is impossible without precise clinical documentation. The coder can only assign codes based on what the provider has documented.
What Providers Must Document for Accurate Coding:
-
A Clear Etiology: “Diabetic neuropathy,” “postherpetic,” “chemotherapy-induced,” “post-traumatic.”
-
The Specific Type of Neuropathy: “Polyneuropathy,” “mononeuropathy,” “radiculopathy,” “causalgia.”
-
Laterality: Right, left, or bilateral.
-
The Chronic Nature: Explicit use of the term “chronic” if applicable.
-
Specific Syndromes: “Complex Regional Pain Syndrome,” “Central Pain Syndrome,” “Phantom Limb Pain with pain.”
-
Linkage: Clearly linking the pain to the underlying condition.
The Query Process: If the documentation is unclear or conflicting (e.g., the assessment says “neuropathic pain” but the plan references “low back pain”), the coder must initiate a formal query to the provider to clarify the diagnosis before assigning a code.
Chapter 8: Beyond ICD-10 – The Impact of Accurate Coding
The consequences of precise coding extend far beyond a clean claim.
-
Reimbursement: Accurate codes ensure that the provider’s work in managing these complex conditions is properly valued and reimbursed. Undercoding leads to lost revenue; overcoding or incorrect coding can lead to audits, denials, and penalties.
-
Population Health: Health systems and researchers use coded data to identify populations with specific conditions, like diabetic neuropathy, to target outreach programs, manage resources, and measure outcomes.
-
Research and Drug Development: Pharmaceutical companies and clinical researchers rely on accurate coded data to identify potential patients for clinical trials for new neuropathic pain medications.
-
The Future – ICD-11: The WHO’s ICD-11, which is gradually being adopted, has a more refined structure for chronic pain. It includes a dedicated parent code (MG30) for Chronic Pain, with subcategories for Chronic neuropathic pain (MG30.0). This promises a more intuitive and direct coding system for these conditions in the future, moving closer to recognizing neuropathic pain as a distinct diagnostic entity.
Conclusion
Navigating the ICD-10 coding for neuropathic pain requires a dual expertise in coding guidelines and clinical knowledge. There is no single code, but a logical pathway defined by etiology. The coder must first identify the underlying cause of the nerve damage, assign the most specific code for that condition, and then judiciously apply additional codes for the pain itself only when necessary and supported by documentation. By mastering this process, healthcare professionals ensure financial integrity, contribute to valuable health data, and, most importantly, help accurately represent the profound burden shouldered by patients living with neuropathic pain.
Frequently Asked Questions (FAQs)
Q1: Is there a single ICD-10 code just for “neuropathic pain”?
A: No. ICD-10 requires coding the underlying cause (e.g., diabetes, shingles, nerve injury). The neuropathic pain is considered a symptom or manifestation of that underlying condition.
Q2: When should I use a code from the G89 category (like G89.29 or G89.4) for a neuropathic pain patient?
A: Use a G89 code when the provider’s documentation specifically identifies “chronic pain” or “chronic pain syndrome” as a condition being managed separately from the underlying cause. It is often used when the pain itself is the primary focus of treatment, even if the initial cause is known. Do not use it if the code for the underlying condition already describes a painful neuropathy (e.g., B02.29 for PHN).
Q3: A patient has diabetic neuropathy (E11.42) and the pain is severe and chronic. Can I code E11.42 and G89.29 together?
A: It is possible, but you must follow coding guidelines and payer-specific rules. The code E11.42 already implies a painful condition. Adding G89.29 may be acceptable if the documentation specifically states that the “chronic pain” is a separate, additional problem being addressed. However, many payers may see this as redundant. The safest practice is to code only E11.42 unless there is a clear, documented reason to add the G89.29 code, and to follow official guidelines.
Q4: How do I code “small fiber neuropathy” when the cause is unknown?
A: If the etiology is unknown after all testing, you would code G62.9 (Polyneuropathy, unspecified). The provider’s documentation of “small fiber neuropathy” is a specific clinical diagnosis, but without a known cause, it maps to this unspecified code. You would not add a separate pain code.
Q5: What is the difference between G89.29 (Other chronic pain) and G89.4 (Chronic pain syndrome)?
A: G89.29 is a broader code for any chronic pain not classified elsewhere. G89.4 is more specific and typically refers to a complex biopsychosocial condition where the chronic pain has led to significant functional disability and psychological distress (e.g., anxiety, depression). Documentation must explicitly support the use of G89.4.
Additional Resources
-
CDC ICD-10-CM Official Guidelines for Coding and Reporting: The definitive source for coding rules. (https://www.cdc.gov/nchs/icd/icd-10-cm.htm)
Date: October 15, 2025
Author: The Medical Coding Specialist Team
Disclaimer: The information contained in this article is for educational and informational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or coding practice. The codes and guidelines referenced are based on current knowledge and are subject to change.





