Imagine sitting down to enjoy a cherished meal, only to be met with an immediate and unsettling sensation—food sticking in your throat, a persistent gurgling noise with every swallow, and the involuntary return of undigested food minutes or even hours later. For individuals living with Zenker’s Diverticulum, this is not a rare occurrence but a daily, distressing reality. This condition, a pulsion diverticulum of the pharynx, represents a fascinating convergence of anatomy, physiology, and pathology. It is a disorder that challenges the simple, automated act of swallowing, turning it into a complex, often anxiety-inducing process. This article delves deep into the world of Zenker’s Diverticulum, offering an exhaustive exploration of its origins, its clinical footprint, the sophisticated diagnostic tools used to identify it, and the array of modern treatment strategies that can restore the simple pleasure of a meal. We will journey from the microscopic anatomy of the pharyngeal wall to the cutting-edge endoscopic procedures that have revolutionized patient care, providing a definitive resource for patients, caregivers, and medical professionals alike.
icd 10 code zenker’s diverticulum
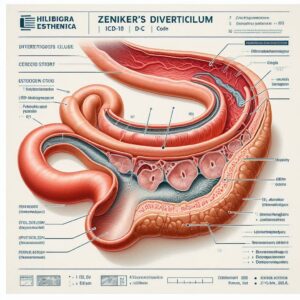
2. What is Zenker’s Diverticulum? Anatomy of a Pouch
At its core, a Zenker’s Diverticulum (ZD) is an outpouching, or sac, that forms in the posterior wall of the hypopharynx. It is not a true diverticulum involving all layers of the wall but rather a “false” or pulsion diverticulum, meaning the mucosal and submucosal layers herniate through the muscular layer. This herniation creates a pouch where food and liquids can become trapped, leading to the condition’s characteristic symptoms.
The Killian’s Triangle: The Locus of Weakness
The genesis of ZD lies in a specific area of anatomical vulnerability known as Killian’s triangle (or Killian’s dehiscence). This is a triangular region in the posterior pharyngeal wall, bounded superiorly by the oblique fibers of the thyropharyngeus muscle (part of the inferior pharyngeal constrictor) and inferiorly by the transverse fibers of the cricopharyngeus muscle. The cricopharyngeus muscle acts as the upper esophageal sphincter (UES), a critical gatekeeper that relaxes to allow food into the esophagus and remains closed at rest to prevent air from entering the gut and refluxate from entering the pharynx. Killian’s triangle is a naturally occurring point of lesser resistance, and under certain conditions, it becomes the site of herniation.
Pathophysiology: The Perfect Storm of Pressure and Resistance
The prevailing theory behind the formation of ZD is a dysfunction of the cricopharyngeus muscle, often described as incomplete relaxation, premature contraction, or hypertonicity (increased resting pressure). This condition is known as cricopharyngeal bar or dysfunction. During the complex coordinated act of swallowing, the UES must relax completely to allow the food bolus to pass seamlessly into the esophagus. If the cricopharyngeus fails to relax appropriately, it creates a functional obstruction. The pharyngeal muscles must then generate increased intraluminal pressure to force the bolus through this resistant sphincter. Over time, this elevated pressure, repeatedly exerted against the weak spot of Killian’s triangle, causes the mucosa and submucosa to bulge through, eventually forming a permanent sac—the Zenker’s diverticulum. As the diverticulum enlarges, it hangs posterior to the esophagus, and food preferentially enters the pouch due to gravity, exacerbating the symptoms.
ICD-10 Code: K22.5 – Demystifying the Classification
In the standardized language of medical classification, the ICD-10 code for Zenker’s Diverticulum is K22.5. Understanding this code is essential for healthcare administration, billing, and research.
-
ICD-10: The International Classification of Diseases, 10th Revision, is a global system used to code all diagnoses, symptoms, and procedures.
-
Category K22: This category is designated for “Other diseases of esophagus.”
-
Code K22.5: This specific code stands for “Diverticulum of esophagus, acquired.” It is important to note that while Zenker’s is anatomically a pharyngeal diverticulum, it is classified under esophageal diseases in the ICD-10 system. This code distinguishes it from other types of esophageal diverticula, such as epiphrenic or traction diverticula.
3. Epidemiology and Risk Factors: Who is Affected?
Zenker’s Diverticulum is a condition that predominantly manifests later in life. It is most frequently diagnosed in individuals over the age of 60, with the incidence increasing with advancing age. It is relatively uncommon, with an estimated incidence of 1 to 2 per 100,000 people per year. There is a noted male predominance, with men being affected approximately 2-3 times more often than women.
While the exact cause of cricopharyngeal dysfunction is not always clear, several factors are associated with an increased risk of developing ZD:
-
Age: The primary risk factor. The muscles and connective tissues of the pharynx can weaken with age, and the cumulative effect of a lifetime of swallowing may contribute to the failure of Killian’s triangle.
-
Gender: The male predisposition is not fully understood but may be related to anatomical or lifestyle differences.
-
Comorbidities: Conditions associated with esophageal dysmotility or increased resistance at the UES may play a role. These include:
-
Gastroesophageal Reflux Disease (GERD): Chronic reflux is thought to contribute to inflammation and spasm of the cricopharyngeus.
-
Hiatal Hernia
-
Other esophageal motility disorders.
-
4. Clinical Presentation: The Telltale Signs and Symptoms
The symptoms of Zenker’s Diverticulum are progressive, often starting insidiously and worsening as the diverticulum enlarges. Patients may adapt their eating habits for years before seeking medical attention, attributing their difficulties to “getting older.”
The Classic Triad: Dysphagia, Regurgitation, and Cervical Borborygmi
-
Dysphagia (Difficulty Swallowing): This is the most common symptom. Patients report a sensation of food, particularly solids, “getting stuck” in the lower neck region. They may need to swallow repeatedly, wash food down with large amounts of liquid, or perform specific maneuvers like neck extension or coughing to empty the pouch.
-
Regurgitation: This is the passive, effortless return of undigested food, often occurring minutes to hours after a meal. Unlike vomiting, there is no associated nausea or retching. The regurgitated material is recognizable as food and may be accompanied by copious saliva. A pathognomonic feature is nocturnal regurgitation, which can lead to aspiration pneumonia if the material is inhaled into the lungs while sleeping.
-
Cervical Borborygmi (Gurgling Noises): Patients may hear audible gurgling or gushing sounds in their neck during or after swallowing. This is caused by the movement of air and fluid within the diverticular pouch.
Beyond the Basics: Halitosis, Aspiration, and Weight Loss
-
Halitosis (Bad Breath): The retention and fermentation of food particles in the pouch can lead to profoundly foul-smelling breath.
-
Aspiration and Respiratory Complications: The overflow of pouch contents into the larynx can cause coughing, choking, and recurrent respiratory infections like bronchitis or pneumonia.
-
Weight Loss and Malnutrition: As dysphagia worsens, patients may unconsciously reduce their food intake, leading to significant, unintentional weight loss and nutritional deficiencies.
-
Globus Sensation: A persistent feeling of a “lump in the throat” even when not swallowing.
-
Voice Changes: A “wet” or gurgly quality to the voice (phonation) due to the presence of secretions in the pouch.
5. The Diagnostic Odyssey: From Clinical Suspicion to Confirmation
A strong clinical history is often the first step toward diagnosis. When a patient presents with the classic triad, suspicion for ZD is high. The diagnostic pathway is designed to confirm the presence of the pouch, assess its size and location, and evaluate the underlying motility disorder.
The Gold Standard: Barium Swallow Study
The barium swallow (or videofluoroscopic swallow study) is the definitive diagnostic test for Zenker’s Diverticulum. The patient swallows a liquid contrast material (barium), and real-time X-ray (fluoroscopy) is used to visualize the swallowing process. A Zenker’s diverticulum appears as a characteristic barium-filled pouch projecting posteriorly from the hypopharynx, typically at the C5-C6 vertebral level. The study beautifully demonstrates the filling of the pouch, its retention of contrast, and the often-seen narrowing at the level of the cricopharyngeus muscle. It also allows for measurement of the diverticulum’s size, which can guide treatment decisions.
(Image: A lateral-view X-ray from a barium swallow study clearly showing a large, barium-filled Zenker’s diverticulum projecting posteriorly from the esophagus.)
The Role of Flexible Endoscopy: A Cautionary View
Transnasal or transoral flexible laryngoscopy or esophagoscopy is frequently performed but must be done with extreme caution. The endoscopist may see a “pulsion” or bulging of the posterior pharyngeal wall, and pooling of secretions in the hypopharynx. However, the opening of the diverticulum (the ostium) can often be mistaken for the true esophageal inlet. Advancing the scope into the diverticulum carries a high risk of perforation. Therefore, endoscopy is used more for ruling out other pathologies and is not the primary diagnostic tool for ZD.
High-Resolution Manometry: Unveiling the Motility Defect
While not required for diagnosis, high-resolution manometry (HRM) is an invaluable tool for understanding the pathophysiology. It involves placing a catheter with multiple pressure sensors through the nose and into the esophagus. During swallows, it provides a detailed color-coded pressure map of the pharynx and esophagus. HRM can objectively identify the high resting pressure and/or failed relaxation of the UES that is the root cause of the diverticulum.
6. Navigating Treatment Options: A Spectrum of Interventions
Treatment for Zenker’s Diverticulum is indicated for all symptomatic patients. The goal of all interventions is twofold: 1) to eliminate the pouch as a reservoir for food, and 2) to ablate the cricopharyngeal bar that caused it. The choice of procedure depends on the diverticulum’s size, patient comorbidities, surgeon expertise, and available technology.
Observation and Conservative Management: When to Wait and See
For very small, asymptomatic diverticula discovered incidentally, observation may be an option. Dietary modifications, such as chewing thoroughly, eating slowly, and drinking plenty of fluids during meals, may provide temporary symptomatic relief for some, but they do not address the underlying anatomical problem.
The Endoscopic Revolution: Stapling, Laser, and Coblator Techniques
Endoscopic techniques have become the first-line treatment for most patients due to their minimally invasive nature, shorter operative times, and faster recovery.
-
Endoscopic Stapled Diverticulostomy (Dohlman’s Procedure): This is the most common endoscopic approach. Under general anesthesia, a specially designed laryngoscope (diverticuloscope) is used to expose the common wall between the esophagus and the diverticulum—the “party wall” that contains the cricopharyngeal bar. A surgical stapler is then deployed to simultaneously cut and staple this common wall. This creates a single, large lumen, allowing food to pass freely and preventing it from entering the pouch. The main limitation is that it is best suited for diverticula of at least 2-3 cm in length to allow for proper placement of the stapler.
-
Laser or Coblator Diverticulostomy: For smaller diverticula where a stapler cannot be used, the common wall can be divided using a CO2 laser or a coblator plasma device. These tools precisely cut through the cricopharyngeal bar, achieving the same physiological result as the stapling procedure.
Traditional Open Surgery: Diverticulectomy with Cricopharyngeal Myotomy
Open surgery, performed through an incision in the neck, was the historical gold standard and is still an excellent option, particularly for very large diverticula or when endoscopic access is difficult.
-
Diverticulectomy: This involves surgically dissecting and completely removing the diverticular pouch.
-
Cricopharyngeal Myotomy: A crucial component of the procedure, this involves cutting the cricopharyngeus muscle longitudinally to relieve the functional obstruction.
-
Diverticulopexy: An alternative to removal, where the pouch is suspended and sutured upside down so it cannot fill with food.
While highly effective, open surgery carries higher risks, including injury to the recurrent laryngeal nerve (causing hoarseness), pharyngocutaneous fistula (a leak from the pharynx to the skin), and longer hospital stays.
Peroral Endoscopic Myotomy (Z-POEM): The New Frontier
The latest advancement is a technique adapted from POEM used for achalasia. In Z-POEM (Zenker’s Peroral Endoscopic Myotomy), an endoscope is used to create a tunnel within the submucosal layer of the esophageal wall, approach the cricopharyngeal bar from beneath, and divide it. This is a truly incisionless, natural orifice transluminal endoscopic surgery (NOTES) procedure with promising early results, though its long-term efficacy is still being evaluated.
Comparing Primary Treatment Modalities for Zenker’s Diverticulum
| Feature | Endoscopic Stapling | Open Surgery (Diverticulectomy) | Z-POEM |
|---|---|---|---|
| Invasiveness | Minimally Invasive | Invasive (neck incision) | Incisionless (Natural Orifice) |
| Anesthesia | General | General | General |
| Procedure Goal | Divide common wall (stapling/laser) | Remove pouch + divide muscle | Create submucosal tunnel & divide muscle |
| Hospital Stay | Short (1-2 days) | Longer (3-5 days) | Short (1-2 days) |
| Recovery Time | Fast (days) | Slower (weeks) | Fast (days) |
| Advantages | Lower complication rate, faster return to diet | Definitive for very large pouches | No external scars, suitable for challenging anatomy |
| Disadvantages | Limited by pouch size (<2cm), recurrence risk | Higher risk of nerve injury, fistula, infection | Newer procedure, long-term data pending, technically demanding |
| Ideal For | Most patients with pouches >2-3 cm | Very large pouches, revision cases, failed endoscopic therapy | Patients seeking incisionless option, smaller pouches |
7. The Post-Procedure Journey: Recovery, Outcomes, and Potential Complications
Recovery varies significantly by procedure. After endoscopic techniques, patients are typically started on a liquid diet the same day, advancing to soft foods and then a regular diet within a week. Most can go home within 24-48 hours. Recovery from open surgery is more protracted, with a longer period of dietary restriction and neck care.
Overall, the success rates for symptomatic relief are high, exceeding 90% for both endoscopic and open approaches. The most common long-term issue is recurrence of symptoms, which occurs in 5-15% of patients and may require a repeat procedure.
Potential complications, though uncommon, include:
-
Perforation/Leak: A leak from the pharyngeal suture or staple line.
-
Mediastinitis: A serious infection of the chest cavity if a leak occurs.
-
Recurrent Laryngeal Nerve Injury: Leading to hoarseness and, rarely, breathing difficulty.
-
Dental Injury: From instrumentation during endoscopic procedures.
-
Bleeding.
8. Living with Zenker’s Diverticulum: Diet, Lifestyle, and Quality of Life
For patients awaiting treatment or managing mild symptoms, certain strategies can help:
-
Dietary Adjustments: Eat small, frequent meals. Chew food thoroughly. Drink carbonated beverages or water during meals to help flush the pouch. Avoid tough meats, bread, and sticky foods like rice.
-
Postural Techniques: Swallowing with the chin tucked or turning the head to the side can sometimes help direct food away from the pouch.
-
Emptying the Pouch: Some patients learn to manually compress their neck to empty the diverticulum after eating (though this is not a long-term solution).
The impact of successful treatment on quality of life is profound. The relief from dysphagia, the elimination of embarrassing regurgitation and gurgling, and the freedom to eat without fear can be transformative.
9. Conclusion: Synthesizing the Journey
Zenker’s Diverticulum is a condition born from a specific anatomical weakness and a functional obstruction at the upper esophageal sphincter. Its diagnosis is elegantly confirmed by a barium swallow, which reveals the telltale posterior pouch. Modern treatment has shifted decisively towards minimally invasive endoscopic techniques that effectively eliminate the pouch and its cause, offering patients rapid relief and recovery with minimal risk. With accurate diagnosis and appropriate intervention, the profound disruption to swallowing and quality of life caused by this condition can be successfully resolved.
10. Frequently Asked Questions (FAQs)
Q1: Is Zenker’s Diverticulum a form of cancer?
A: No, Zenker’s Diverticulum is a benign condition. It is a pouch formed from the lining of the pharynx. However, in extremely rare cases (less than 0.5%), long-standing, untreated diverticula can undergo malignant transformation, which is one reason why treatment is recommended for symptomatic patients.
Q2: Can Zenker’s Diverticulum be treated with medication or diet alone?
A: No. While dietary changes can help manage symptoms temporarily, they do not address the underlying anatomical problem—the pouch and the dysfunctional muscle. The only definitive treatment is a procedure to divide the cricopharyngeal bar and eliminate the pouch as a reservoir.
Q3: What happens if Zenker’s Diverticulum is left untreated?
A: Symptoms will almost certainly progress. The diverticulum typically enlarges over time, leading to worsening dysphagia, significant weight loss and malnutrition, and an increased risk of life-threatening complications like aspiration pneumonia.
Q4: How do I know if my symptoms are from Zenker’s or just bad reflux?
A: While both can cause regurgitation, the nature of the regurgitated material is key. Zenker’s typically involves regurgitation of undigested, recognizable food that tastes normal, occurring minutes to hours after a meal. GERD-related regurgitation usually involves partially digested food mixed with acidic stomach juices, causing a sour or bitter taste, and is more closely tied to heartburn.
Q5: Is the treatment for Zenker’s Diverticulum considered major surgery?
A: It depends on the approach. Traditional open surgery is considered a major operation. However, the now-standard endoscopic approaches are minimally invasive procedures, often performed as same-day or 23-hour stays, with a much faster recovery and are not considered “major” in the traditional sense.
11. Additional Resources
-
The American Gastroenterological Association (AGA): Provides patient-centered information on digestive diseases.
-
The American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS): Offers resources on conditions of the throat and swallowing, often from a surgical perspective.
-
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): A part of the NIH, providing comprehensive, evidence-based information on digestive disorders.
-
ClinicalTrials.gov: A database of publicly and privately supported clinical studies conducted around the world, for those interested in ongoing research.
Date: November 15, 2025
Author: Dr. Alistair Finch
Disclaimer: The information contained in this article is intended for educational and informational purposes only and does not constitute medical advice. It is not a substitute for professional medical diagnosis, treatment, or care. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition.





