In the modern healthcare ecosystem, a patient’s journey is narrated through two parallel stories: one of clinical care, written in physician notes and operative reports, and one of data, etched in alphanumeric codes. For the millions of patients diagnosed with uterine myomas—the most common pelvic tumor in people with uteruses—the procedural intervention they undergo must be meticulously translated into a specific, standardized language. This language is ICD-10-PCS (International Classification of Diseases, Tenth Revision, Procedure Coding System), and mastery of it is not merely an administrative task; it is a critical function that fuels healthcare reimbursement, shapes public health understanding, drives clinical research, and ensures the integrity of medical records.
This article embarks on a deep, exhaustive exploration of ICD-10-PCS coding for uterine myoma procedures. We will move beyond simple code lookup and delve into the logic, structure, and clinical nuances that inform accurate code selection. From a diagnostic hysteroscopy to a radical abdominal hysterectomy, each intervention tells a distinct story through its PCS code. Our journey will equip medical coders, healthcare administrators, clinical professionals, and interested patients with a detailed map to navigate this complex but essential terrain, emphasizing the “why” behind the “what” of procedural coding.
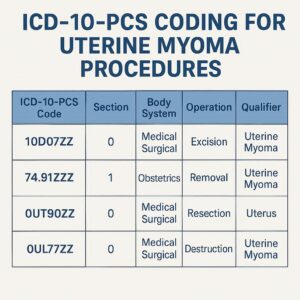
ICD-10-PCS coding for uterine myoma procedures
2. Understanding the Foundation: Uterine Myomas (Fibroids)
Before a single code can be assigned, a firm grasp of the clinical entity is paramount. Uterine myomas, or leiomyomas, are benign monoclonal tumors arising from the smooth muscle cells of the myometrium. Their prevalence is staggering, affecting an estimated 70-80% of people with uteruses by age 50. While often asymptomatic, myomas can be the source of debilitating symptoms: heavy menstrual bleeding (menorrhagia) leading to anemia, pelvic pain or pressure, urinary frequency, constipation, and reproductive challenges such as infertility or recurrent pregnancy loss.
The management of myomas is dictated by symptom severity, patient age, desire for future fertility, and the size, number, and location of the tumors. Location is particularly crucial from both a clinical and coding perspective:
-
Submucosal: Project into the endometrial cavity. Often cause abnormal bleeding and are frequently addressed via hysteroscopic resection.
-
Intramural: Embedded within the myometrial wall. The most common type.
-
Subserosal: Project outward from the serosal surface of the uterus. Can become pedunculated.
-
Cervical: Located in the cervix.
This anatomical distinction directly influences the choice of procedure and, consequently, the PCS code.
3. ICD-10-PCS vs. ICD-10-CM: A Fundamental Distinction
A common point of confusion is the difference between the two ICD-10 code sets used in the United States.
-
ICD-10-CM (Clinical Modification): Used for diagnosis coding. It answers “Why was the patient treated?” For uterine myomas, the relevant diagnosis code is typically D25.9 (Leiomyoma of uterus, unspecified) or more specific codes like D25.0 (Submucosal leiomyoma), D25.1 (Intramural leiomyoma), and D25.2 (Subserosal leiomyoma).
-
ICD-10-PCS (Procedure Coding System): Used exclusively for inpatient procedure coding in hospital settings. It answers “What was done to the patient?” This is our primary focus. It describes the specific surgical or medical procedure performed, such as an excision, resection, or destruction of the myoma tissue.
4. Navigating the ICD-10-PCS Structure: The 7-Character Code
ICD-10-PCS is built on a logical, multi-axial structure. Every procedure is represented by a unique 7-character alphanumeric code. Each character has a specific meaning, and together they provide a highly detailed description of the procedure.
The 7 Characters:
-
Section: The broadest category (e.g., Medical and Surgical, Obstetrics).
-
Body System: The physiological system or anatomical region (e.g., Female Reproductive System).
-
Root Operation: The objective of the procedure (e.g., Cutting out vs. Taking out).
-
Body Part: The specific anatomical site (e.g., Uterus, Endometrium).
-
Approach: The technique used to reach the site (e.g., Open, Percutaneous, Via Natural Opening).
-
Device: Any device left in place (e.g., Monitoring Device, Radioactive Element).
-
Qualifier: An additional attribute for further specificity (e.g., Diagnostic, Myometrium).
5. The Heart of the Matter: The Medical and Surgical Section (0)
The vast majority of uterine myoma procedures fall under the Medical and Surgical Section, identified by the first character 0. The second character for these procedures is almost always U for Female Reproductive System.
6. Root Operations for Uterine Myoma Procedures: From Excision to Resection
The third character—Root Operation—is the most critical and often the most challenging to determine. It defines the intent of the procedure. For myomas, several root operations are relevant:
-
Excision (B): Cutting out or off, without replacement, a portion of a body part. The qualifier “diagnostic” is often used here.
-
Clinical Example: Laparoscopic myomectomy where a single myoma is shelled out. Also, a hysteroscopic polypectomy/myomectomy of a submucosal myoma.
-
Coding Implication: The body part is the specific site (e.g., Endometrium, Myometrium) from which the myoma is excised.
-
-
Resection (T): Cutting out or off, without replacement, all of a body part.
-
Clinical Example: Total abdominal hysterectomy for multiple large myomas. The entire uterus is removed.
-
Coding Implication: The body part is the organ itself (Uterus).
-
-
Destruction (5): Physical eradication of all or a portion of a body part by the direct use of energy, force, or a destructive agent.
-
Clinical Example: Hysteroscopic ablation of a submucosal myoma using electrical energy (e.g., resectoscope) or laser. The myoma tissue is destroyed, not physically removed.
-
Coding Implication: No specimen may be sent to pathology. The body part is the site of destruction.
-
-
Extirpation (C): Taking or cutting out solid matter from a body part.
-
Clinical Example: This is less common for myomas but could theoretically apply to a procedure focused solely on removing a calcified myoma fragment.
-
-
Occlusion (L): Completely closing an orifice or lumen of a tubular body part.
-
Clinical Example: Uterine artery embolization (UAE). The objective is to occlude the uterine arteries to starve the myomas of blood supply.
-
Coding Implication: The body part is the uterine artery, not the uterus.
-
Key ICD-10-PCS Root Operations for Uterine Myoma Management
| Root Operation | Definition (PCS Official) | Common Myoma Procedure | Key Distinction |
|---|---|---|---|
| Excision (B) | Cutting out or off a portion of a body part | Myomectomy, Polypectomy | Portion is removed; specimen sent to pathology. |
| Resection (T) | Cutting out or off all of a body part | Hysterectomy | Entire organ is removed. |
| Destruction (5) | Eradicating without physical removal | Hysteroscopic Ablation | Uses energy/force; may be no specimen. |
| Occlusion (L) | Closing an orifice/lumen | Uterine Artery Emolization (UAE) | Target is the feeding vessel, not the myoma itself. |
7. The Approach Character: A Tale of Invasiveness
The fifth character defines the Approach. This is a key differentiator in modern gynecology, impacting recovery time and coding.
-
Open (0): Cutting through skin or mucous membrane and directly visualizing the surgical field (e.g., abdominal hysterectomy via Pfannenstiel or midline incision).
-
Percutaneous (3): Entry by puncture or minor incision, often using imaging guidance (e.g., UAE, where a catheter is threaded through the femoral artery).
-
Percutaneous Endoscopic (4): Percutaneous entry with the use of a scope for visualization (e.g., laparoscopic myomectomy or hysterectomy).
-
Via Natural or Artificial Opening (7): Entry through a natural orifice (e.g., vagina, urethra) or a pre-existing artificial opening.
-
Via Natural or Artificial Opening Endoscopic (8): Entry through a natural/artificial opening with the use of a scope (e.g., hysteroscopic myomectomy or ablation—the scope passes through the vagina and cervix).
8. Device and Qualifier: Finishing the Code
-
Device (6th Character): For myoma procedures, this is often Z (No Device). Exceptions include UAE, where an embolization coil or other embolic material is left implanted, or procedures involving temporary monitoring devices.
-
Qualifier (7th Character): Provides essential final detail.
-
Diagnostic (X): Used when the primary purpose of the excision or biopsy is to obtain tissue for pathology.
-
Myometrium (1): A specific qualifier under the “Endometrium” body part to indicate a procedure was focused on the underlying muscle layer where myomas reside (e.g., 0UBD8ZX for a hysteroscopic excision of myometrial tissue).
-
9. The Obstetrics Section (1): A Special Consideration
Procedures performed during a delivery or for obstetric indications use the Obstetrics Section. A cesarean hysterectomy for a uterus rendered unstable by myomas would be found here (e.g., 10T00Z1 for a classical cesarean hysterectomy). Coders must carefully review the operative report to determine if the procedure’s intent is purely obstetric.
10. Putting It All Together: Common Procedure Scenarios and Codes
Scenario 1: Laparoscopic Myomectomy (Excision of multiple intramural myomas)
-
Section/System: 0U (Medical and Surgical, Female Reproductive System)
-
Root Operation: B (Excision)
-
Body Part: U (Uterus) or 1 (Myometrium) — depends on coder interpretation and facility-specific guidelines.
-
Approach: 4 (Percutaneous Endoscopic)
-
Device: Z (No Device)
-
Qualifier: Z (No Qualifier)
-
Potential Code: 0UB94ZZ (Excision of Uterus, Percutaneous Endoscopic Approach)
Scenario 2: Total Abdominal Hysterectomy for Leiomyomas (Resection of the entire uterus)
-
Section/System: 0U
-
Root Operation: T (Resection)
-
Body Part: U (Uterus)
-
Approach: 0 (Open)
-
Device: Z
-
Qualifier: Z
-
Code: 0UT90ZZ
Scenario 3: Hysteroscopic Myomectomy/Resection of a Submucosal Myoma
-
Section/System: 0U
-
Root Operation: B (Excision) or 5 (Destruction) if ablated.
-
Body Part: M (Endometrium) — as the myoma projects into the cavity.
-
Approach: 8 (Via Natural or Artificial Opening Endoscopic)
-
Device: Z
-
Qualifier: 1 (Myometrium) if the root is in the muscle.
-
Potential Code (for excision): 0UBM8ZX (Excision of Endometrium, Via Natural Opening Endoscopic, Diagnostic)
Scenario 4: Uterine Artery Embolization (UAE)
-
Section/System: 04 (Medical and Surgical, Lower Arteries)
-
Root Operation: L (Occlusion)
-
Body Part: 3 (Uterine Artery)
-
Approach: 3 (Percutaneous)
-
Device: Y (Intraluminal Device, e.g., embolic coils)
-
Qualifier: Z
-
Code: 04L33ZY
11. The Impact of Accurate Coding: Reimbursement, Research, and Audits
Precise PCS coding is not an academic exercise. It is the linchpin of the hospital revenue cycle, determining Diagnosis-Related Group (DRG) assignment and subsequent reimbursement. Inaccurate coding can lead to underpayment, denials, or allegations of fraud. Furthermore, this coded data is aggregated for vital public health statistics, clinical outcomes research, and quality benchmarking. An audit that finds inconsistent or incorrect coding can result in significant financial penalties and reputational damage.
12. Conclusion
Navigating ICD-10-PCS coding for uterine myoma procedures requires a systematic fusion of clinical knowledge and coding expertise. By meticulously analyzing the operative report to identify the correct root operation, body part, and approach, coding professionals translate complex surgical interventions into precise, standardized data. This data integrity is the unsung foundation of a functional, accountable, and knowledge-driven healthcare system.
13. Frequently Asked Questions (FAQs)
Q1: What is the most common ICD-10-PCS code for a myomectomy?
A: There is no single “most common” code, as it depends on the approach. For an open abdominal myomectomy, it’s often 0UB90ZZ. For a laparoscopic myomectomy, it’s 0UB94ZZ. For a hysteroscopic myomectomy, it’s typically 0UBM8ZX.
Q2: How do I code a robotic-assisted laparoscopic hysterectomy for fibroids?
A: In ICD-10-PCS, the robotic platform is not specified in the code. A robotic-assisted procedure is coded to the approach it mimics, which is Percutaneous Endoscopic (4). Therefore, a robotic total hysterectomy is coded identically to a laparoscopic one: 0UT94ZZ.
Q3: What is the difference between excision (B) and resection (T) of the uterus?
A: This is a crucial distinction. Excision (B) of the uterus refers to removing a portion of it, like in a myomectomy or wedge resection. Resection (T) means removing the entire uterus, as in a total hysterectomy.
Q4: When do I use the “Diagnostic” qualifier?
A: Use the qualifier Diagnostic (X) when the procedure’s sole purpose is to obtain tissue for pathologic analysis and no definitive therapeutic treatment is performed at that time. If a myoma is excised for both treatment and diagnosis, the qualifier is generally not used.
Q5: Where can I find the official coding guidelines?
A: The definitive resources are the annual ICD-10-PCS code book published by the Centers for Medicare & Medicaid Services (CMS) and the American Hospital Association (AHA) Coding Clinic for ICD-10-CM/PCS.
Date: December 13, 2025
Author: Clinical Coding Specialist
Disclaimer: This article is for educational and informational purposes only. It is not a substitute for professional medical coding advice. Always consult the official ICD-10-PCS code books, guidelines, and payer-specific policies for definitive coding instruction.





