If you or your child have been diagnosed with a tongue-tie (ankyloglossia), you are likely navigating a world of new terminology, treatment options, and—most confusingly—insurance codes.
One of the first questions that comes up during treatment planning is usually about the cost. But before you can understand the cost, you need to understand the language of dental billing.
The dental code for lingual frenectomy is not always a single, straightforward number. Depending on the severity of the condition, the method used (scalpel vs. laser), and whether the procedure is performed by a dentist, oral surgeon, or pediatrician, the code can change.
This guide is designed to clear up the confusion. We will walk you through the specific Current Dental Terminology (CDT) codes used for this procedure, explain what each code actually covers, and help you understand what to expect when the bill arrives.
Whether you are a dental professional looking for clarity on coding guidelines or a patient trying to decipher your treatment plan, this article provides a realistic, honest look at how lingual frenectomies are coded and billed in the United States.
Dental Code for Lingual Frenectomy
What Exactly is a Lingual Frenectomy?
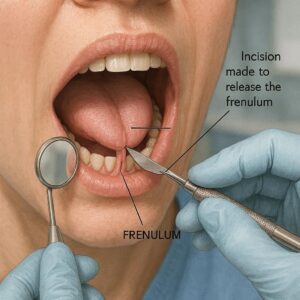
Before we dive into the numbers and billing nuances, it helps to have a clear picture of the procedure itself. A lingual frenectomy is a simple surgical procedure designed to correct a condition known as ankyloglossia, or “tongue-tie.”
The lingual frenum is a small band of tissue that connects the underside of the tongue to the floor of the mouth. In a healthy mouth, this band allows the tongue to move freely—essential for speech, eating, and swallowing.
When this frenum is too short, thick, or tight, it restricts the tongue’s range of motion.
Why is this procedure necessary?
For infants, a tongue-tie can make breastfeeding difficult. It can lead to poor latch, nipple pain for the mother, and inadequate nutrition for the baby.
For older children and adults, the implications are broader. A restricted tongue can cause:
-
Speech impediments: Difficulty pronouncing certain consonants like “t,” “d,” “z,” “s,” and “r.”
-
Oral hygiene issues: An inability to sweep food debris from the teeth can lead to cavities and gum disease.
-
Orthodontic problems: A tight frenum can cause a gap between the lower front teeth or alter jaw development.
-
Social discomfort: In severe cases, it can affect kissing or licking one’s lips.
The frenectomy releases this tissue, allowing for a full range of motion. In the dental world, this procedure falls squarely under the umbrella of oral surgery.
The Primary Dental Code for Lingual Frenectomy: D7960
When you look at a dental insurance claim or a treatment estimate, the code you will most frequently see is D7960.
This is the standard CDT code recognized by the American Dental Association (ADA). It is defined as: Frenulectomy (frenectomy or frenotomy) — separate procedure.
Let’s break down what that definition actually means in practice.
What Does “Separate Procedure” Mean?
In the context of dental coding, “separate procedure” is a crucial phrase. It indicates that the frenectomy is the primary reason for the visit. It is not a minor part of a larger, more complex surgery.
For example, if a patient is having a large cyst removed and the surgeon incidentally snips a tight frenum during that procedure, you would not bill D7960 separately. However, if the patient comes in specifically to have their tongue-tie released, and that is the main focus of the appointment, D7960 is the correct code.
What D7960 Typically Covers
When a dentist or oral surgeon bills D7960, it generally includes:
-
Pre-procedural evaluation: The clinical assessment of the frenum and the tongue’s range of motion.
-
Administration of local anesthesia: Numbing the area to ensure patient comfort.
-
The surgical release: The actual cutting or lasering of the tissue.
-
Immediate post-operative care: Instructions given to the patient or caregiver regarding wound care, stretches, and follow-up.
It is important to note that D7960 is a “surgical” code. It does not typically cover the cost of the consultation visit (which is often billed separately under an exam code like D0150 or D0140).
Laser vs. Scalpel: Does the Code Change?
One of the most common sources of confusion is whether the dental code for lingual frenectomy changes depending on the instrument used.
Here is the honest truth: The code does not change based on the instrument.
Whether the surgeon uses a traditional scalpel, surgical scissors, or a soft-tissue laser (such as a CO2 or diode laser), the standard code remains D7960.
Why the Confusion Exists?
The confusion arises from the cost. Laser frenectomies often have a higher out-of-pocket cost than scalpel frenectomies. This is not because the billing code is different, but because:
-
Technology fees: Lasers are expensive equipment that require maintenance and specialized training.
-
Operating efficiency: Lasers often result in less bleeding and faster healing, which many patients feel justifies a premium.
-
Insurance reimbursement: Dental insurance companies usually reimburse the same base amount for D7960 regardless of the tool used. If a dentist uses a laser, the patient often pays the difference between the insurance allowance and the provider’s fee.
A Quick Comparison: Laser vs. Scalpel
| Feature | Scalpel Frenectomy (D7960) | Laser Frenectomy (D7960) |
|---|---|---|
| Primary Code | D7960 | D7960 |
| Anesthesia | Usually local anesthetic | Usually local anesthetic |
| Bleeding | Minor to moderate | Minimal to none |
| Sutures | Often required | Rarely required |
| Healing Time | 1–2 weeks | Often faster (a few days) |
| Patient Experience | Traditional surgical feel | Quieter, often less anxiety |
| Cost | Generally lower | Generally higher |
Important Note: Some providers may attempt to bill a laser frenectomy under a “soft tissue management” code (such as D4999, an unspecified code). However, this is generally not considered standard practice. For a true frenectomy, D7960 is the appropriate and expected code.
Pediatric vs. Adult Coding: D7961 and D7963
While D7960 is the “workhorse” code for frenectomies, the ADA introduced specific codes to address the growing need for more precise reporting, particularly in pediatric dentistry and orthodontics.
If you are looking at a treatment plan for a child or for a frenectomy performed in conjunction with orthodontic work, you might encounter these additional codes.
D7961: Frenulectomy (frenectomy or frenotomy) – Infant
This code was created specifically to address the unique needs of newborn and infant frenectomies (usually under 12 months of age).
Why does this code exist separately?
Infant frenectomies are fundamentally different from adult procedures. They often:
-
Do not require local anesthesia (or use topical only).
-
Are performed quickly, often in a matter of seconds.
-
Involve extensive lactation counseling and post-op follow-up regarding feeding.
-
Are frequently billed to medical insurance rather than dental insurance.
When to use D7961:
-
For patients under 1 year of age.
-
When the primary goal is to improve breastfeeding or bottle feeding.
-
When the procedure is performed in a dental office but requires a different workflow than adult surgery.
D7963: Frenuloplasty – For Orthodontic and Surgical Revisions
This code is distinct from the “ectomy” codes. An ectomy usually involves simply cutting or removing the frenum. A plasty implies a more complex reconstruction.
D7963 is defined as: Frenuloplasty (for orthodontic or surgical revision).
What does this involve?
A frenuloplasty is a more advanced procedure. It is used when the frenum is so thick or restrictive that a simple cut is insufficient. It often involves:
-
Z-plasty techniques: A surgical technique that repositions the tissue to lengthen it and prevent reattachment (scarring).
-
Grafting: Occasionally, tissue grafts are used to cover the area.
-
Orthodontic preparation: This is often performed to close a midline diastema (gap between the front teeth) or to prepare for braces.
If your orthodontist mentions that the gap between your teeth won’t close without surgery, they are likely referring to a frenuloplasty (D7963), not a simple frenectomy (D7960).
| Code | Description | Typical Patient | Complexity |
|---|---|---|---|
| D7960 | Frenulectomy (separate procedure) | Children/Adults | Moderate |
| D7961 | Frenulectomy – Infant | Infants (under 12 months) | Low/Moderate |
| D7963 | Frenuloplasty (orthodontic revision) | Children/Adults | High |
Medical vs. Dental Insurance: Which One Pays?
This is arguably the most critical section of this guide. The success of your insurance claim does not depend solely on which dental code you use; it depends on whether the procedure is considered a medical necessity.
Lingual frenectomies sit in a gray area between dental and medical coverage.
The Medical Insurance Route
Medical insurance (like Blue Cross, Aetna, Cigna Medical) is often the primary payer for frenectomies, particularly in infants or when the issue is tied to functional problems like feeding difficulties.
To get medical insurance to pay, the provider must submit:
-
Medical Codes (ICD-10): These are diagnosis codes that explain why the procedure was done. Common ICD-10 codes for tongue-tie include Q38.1 (Ankyloglossia) and P92.5 (Neonatal difficulty in feeding).
-
Medical Procedure Codes (CPT): Instead of D7960, medical insurance requires CPT (Current Procedural Terminology) codes. The most common CPT code for a frenectomy is 41010 (Incision of lingual frenum). For more complex procedures, 41520 (Frenuloplasty) may be used.
The Dental Insurance Route
Dental insurance typically covers frenectomies if the restriction is affecting dental health, such as causing:
-
Gingival recession (gum recession).
-
Bone loss around the teeth.
-
Difficulty maintaining oral hygiene.
-
Orthodontic relapse.
In this scenario, the provider uses D7960 (or D7963) along with dental-specific diagnosis codes.
The Reality of Coverage
Many patients find themselves in a “coverage gap.”
Some medical insurers deny the claim because they consider it a “dental procedure.” Some dental insurers deny the claim because they consider it “surgical” and beyond their basic coverage.
Here is a realistic expectation:
-
Infants: Medical insurance is usually the primary route. However, not all plans cover it. You must check if your plan has “habilitative” or “feeding” benefits.
-
Adults: Dental insurance is more likely to cover a portion, but many plans have a “missing tooth clause” or exclude “congenital anomalies” (conditions present at birth). Ankyloglossia is congenital, and some plans explicitly exclude coverage for it.
Important Note for Readers: Always ask your provider to verify your benefits before the procedure. Ask specifically: “Will you submit this to my medical or dental insurance? And what is my estimated out-of-pocket cost after insurance?”
The Cost of a Lingual Frenectomy
Since insurance coverage is often inconsistent, it is helpful to understand the typical cash pay (out-of-pocket) costs for these procedures. Keep in mind that prices vary significantly based on geographic location, the specialist performing the work, and the technology used.
Average Price Ranges
| Procedure Type | Typical Code | Estimated Cost (Without Insurance) |
|---|---|---|
| Infant Frenectomy | D7961 / CPT 41010 | $250 – $800 |
| Adult Scalpel Frenectomy | D7960 | $300 – $1,200 |
| Adult Laser Frenectomy | D7960 | $600 – $1,800 |
| Frenuloplasty (Complex) | D7963 / CPT 41520 | $1,000 – $3,000+ |
Note: These costs are estimates. If performed by a specialist (pediatric dentist, periodontist, or oral surgeon), costs tend to be on the higher end of the spectrum.
Why the Wide Range?
-
Laser Technology: As mentioned, laser use increases the fee.
-
Anesthesia: If the patient requires IV sedation or general anesthesia (often for very anxious patients or complex revisions), this adds significant cost, usually billed under separate codes (like D9248).
-
Location: Urban centers with higher overhead costs generally charge more than rural clinics.
Step-by-Step: What to Look For on Your Treatment Plan
When you receive a treatment plan or an insurance estimate, it can feel overwhelming. To help you navigate it, here is a checklist of what to look for regarding the dental code for lingual frenectomy.
-
Identify the Code: Look for the 5-character code starting with “D” (e.g., D7960). Verify that it matches the procedure you discussed with the doctor.
-
Check the Diagnosis: Ensure the diagnosis code listed matches your condition. For a tongue-tie, you should see “Ankyloglossia” or a similar term.
-
Look for Anesthesia Codes: If you are undergoing sedation, check for codes like D9241 (IV sedation) or D9230 (inhalation of nitrous oxide). These are often separate line items.
-
Review the “Provider Fee” vs. “Insurance Allowance”: Your insurance will have a contracted rate. If the provider’s fee is $1,200 but the insurance allowance is $600, you are responsible for the difference if the provider is out-of-network.
-
Ask About Exclusions: If the treatment plan says “Excluded,” ask why. Is it because of a “congenital anomaly exclusion”? Knowing this helps you decide whether to appeal to medical insurance instead.
FAQ: Lingual Frenectomy Coding
Navigating the world of dental codes and insurance can be tricky. Here are answers to some of the most frequently asked questions we receive.
1. Is D7960 the same for upper lip tie (labial frenectomy)?
No. While the procedure is similar, the location matters. A labial frenectomy (upper lip tie) has its own code: D7971. D7960 is specifically reserved for the lingual (tongue) frenum. Billing D7960 for a lip tie is incorrect and will result in a denied claim.
2. Can a general dentist perform a frenectomy and bill D7960?
Yes. A general dentist who has the appropriate training and equipment can perform a frenectomy. You do not need to see a specialist unless the case is complex. However, insurance plans may have different reimbursement rates depending on whether the provider is a general dentist or an oral surgeon.
3. Why was my claim denied if the code was correct?
Even with the correct code (D7960), denials happen for several reasons:
-
Frequency: Insurance often limits this procedure to once per lifetime per arch.
-
Age: Some plans do not cover frenectomies over a certain age unless there is a severe pathology.
-
Missing X-rays: Some dental insurers require radiographic evidence (X-rays) to prove the necessity, even for a soft tissue procedure.
-
Coordination of Benefits: If the patient has both medical and dental insurance, the payer may deny the claim, insisting the other insurance should pay first.
4. Is there a difference between a frenectomy and a frenotomy?
Clinically, the difference is subtle. A frenotomy is usually a simple snip of the frenum, often performed on infants with no sutures. A frenectomy implies the complete removal of the frenum. However, in dental coding, D7960 is used interchangeably for both. The ADA does not distinguish between the two in the code descriptor.
5. Does medical insurance accept D7960?
Generally, no. Medical insurance companies use the CPT coding system, not the CDT system. If you want to use your medical insurance, your provider must submit a claim using the appropriate CPT code (usually 41010) and the correct ICD-10 diagnosis code. Many dental offices are not set up to bill medical insurance, which is why patients often have to pay upfront and seek reimbursement themselves.
Additional Resource
To further assist you in understanding the clinical aspects and post-operative care of this procedure, we recommend reviewing the American Academy of Pediatric Dentistry (AAPD) guidelines.
Resource Link: AAPD – Policy on Tongue-Tie and Lip-Tie
This resource provides a professional, evidence-based look at the diagnostic criteria and clinical considerations for frenectomies in children and adolescents.
Important Notes for Readers
As we wrap up this guide, I want to leave you with a few realistic and honest notes to protect you as a patient or to guide you as a professional.
-
Pre-authorization is your best friend. Do not assume coverage. Always ask the office manager to send a pre-treatment estimate to your insurance. This is a non-binding estimate of what they will pay. It takes time, but it saves you from surprise bills.
-
“Bundled” services. If your dentist is performing a frenectomy along with a full mouth reconstruction or orthognathic surgery, they may not bill D7960 separately. In these cases, the cost of the frenectomy is often “bundled” into the larger surgical code. Ask your surgeon if this applies to you.
-
Lactation consultants. For infants, the success of a frenectomy often depends on post-op exercises (stretches) and follow-up with a lactation consultant. These services are rarely covered by dental insurance but may be covered by medical insurance or health savings accounts (HSAs).
-
Appeals work. If your claim is denied, do not simply accept the first decision. Ask your provider to write a letter of medical necessity. If you have an infant with documented feeding problems, a well-written appeal can often overturn a denial.
Conclusion
Understanding the dental code for lingual frenectomy is more than just memorizing the number D7960. It is about understanding the context in which that code is used, the differences between laser and scalpel procedures, and the complex interplay between dental and medical insurance.
We covered the primary code D7960 and its variations—D7961 for infants and D7963 for complex orthodontic revisions. We explored why costs vary, how insurance companies view these claims, and what you can expect to pay out of pocket. Ultimately, being an informed patient means knowing which questions to ask before the procedure begins.
Whether you are seeking this procedure for yourself or your child, clarity on coding is the first step toward a successful outcome and a stress-free financial experience.
Disclaimer
This article is intended for informational and educational purposes only. It does not constitute medical, dental, or legal advice. Dental and medical coding standards, insurance policies, and fee structures vary by state, provider, and insurance carrier. Readers should consult with their licensed dental or medical provider and their insurance company to verify coverage, codes, and treatment plans specific to their situation.





