If you are currently exploring tooth replacement options, you have likely encountered a world of complex terminology. Between crowns, bridges, abutments, and pontics, the language of modern dentistry can feel overwhelming. For many patients, one term in particular stands out as confusing: the implant pontic.
Understanding the dental code for an implant pontic is not just about satisfying curiosity. It is about transparency. When you know what the code means, you can read your treatment plan accurately, verify insurance coverage, and have an informed conversation with your dentist about the care you are receiving.
In this guide, we will break down everything you need to know about the specific code used to bill for an implant pontic, how it differs from other restorative procedures, and what it means for your budget and oral health journey.
Dental Code for Implant Pontic
What Is an Implant Pontic?
Before we dive into the code itself, it is essential to understand what a pontic is and how it functions within a dental restoration.
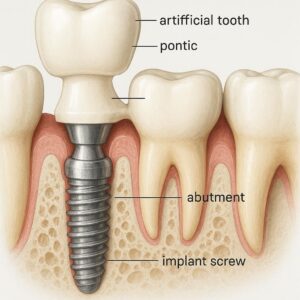
In traditional dentistry, a pontic is the artificial tooth that replaces a missing natural tooth. The word comes from the Latin pons, meaning bridge. In a fixed dental bridge, the pontic is the suspended tooth that fills the gap, anchored by crowns placed on the adjacent natural teeth.
In implant dentistry, the concept shifts slightly. An implant pontic typically refers to a specific type of restoration used in an implant-supported fixed partial denture. Unlike a single implant crown that sits on top of one implant, an implant pontic is used when multiple teeth are being replaced. It is the artificial tooth that sits between two implant abutments or between an implant and a natural tooth abutment, without having its own dedicated implant body directly beneath it.
In simpler terms, imagine you are replacing three missing teeth in a row. Instead of placing three separate implants, a dentist might place two implants—one on each end—and suspend a pontic (the false tooth) in the middle. That middle tooth is the implant pontic.
Why Does This Distinction Matter?
The distinction matters because it determines how the procedure is coded, billed, and reimbursed. An implant that supports a crown uses a different code than an implant that supports a pontic. Knowing this helps you spot why your treatment plan has multiple line items.
The Specific Dental Code: D6064
The official Current Dental Terminology (CDT) code for an implant pontic is D6064.
The full descriptor for this code is: Abutment supported pontic (retained by abutment) for implant/partial denture.
This code is used to describe the fabrication and placement of a pontic that is supported by an abutment connected to a dental implant. The pontic itself does not have its own implant; rather, it relies on the stability provided by adjacent implants or natural teeth via abutments.
Breaking Down the Code
To truly understand D6064, we must look at the components that make up the billing process. This code is part of the implant services section in the CDT manual, which is updated annually by the American Dental Association (ADA).
The code covers:
-
The laboratory fabrication of the pontic (the artificial tooth).
-
The materials used, which are typically high-grade porcelain, zirconia, or a combination of metal and ceramic.
-
The clinical time and skill involved in fitting and seating the pontic onto the abutments.
-
The adjustment and cementation or screw-retention of the pontic to the supporting structure.
It is important to note that D6064 usually does not include the cost of the implant body itself (the screw inserted into the jawbone) or the abutment (the connector piece that attaches to the implant). Those are billed under separate codes.
When Is D6064 Used?
D6064 is specifically used in cases of partial edentulism—where a patient is missing some but not all of their natural teeth. Common scenarios include:
-
Three-unit implant bridge: Two implants placed at the ends with a pontic in the middle.
-
Four-unit implant bridge: Two or more implants supporting multiple pontics.
-
Implant-to-natural tooth bridge: One implant and one natural tooth supporting a pontic (though this is less common today due to biomechanical concerns).
If the pontic were supported by natural teeth only (no implants involved), the correct code would be a traditional fixed partial denture code, such as D6210 or D6245, depending on the material.
A Comparative Overview: Implant Codes vs. Traditional Codes
One of the primary sources of confusion for patients is the difference between implant-supported restorations and traditional tooth-supported restorations. The materials may look similar, but the codes—and therefore the costs and insurance coverage—are vastly different.
| Service Description | Implant-Related Code | Traditional (Tooth-Supported) Code |
|---|---|---|
| Pontic (ceramic) | D6064 (Abutment supported pontic) | D6245 (Pontic, porcelain/ceramic) |
| Abutment placement | D6056 (Prefabricated abutment) or D6057 (Custom abutment) | Not applicable |
| Implant placement | D6010 (Surgical placement) | Not applicable |
| Crown for abutment | D6062 (Abutment supported crown) | D2740 (Porcelain crown) |
As you can see, D6064 sits within a family of codes that work together. If you are having an implant bridge placed, your treatment plan might include:
-
D6010 (Surgical placement of the implants)
-
D6056 (Prefabricated abutment)
-
D6064 (Implant pontic)
-
D6062 (Abutment supported crowns for the implants at the ends)
Understanding this grouping helps you ask the right questions when reviewing your estimate.
The Clinical Workflow: From Surgery to Pontic
To truly appreciate what D6064 represents, it helps to walk through the clinical steps that lead to the placement of an implant pontic. This process is not instantaneous; it requires careful planning and patience.
Phase 1: Diagnosis and Planning
Before any codes are billed, your dentist will perform a comprehensive examination. This includes:
-
Radiographic imaging: Cone beam CT scans to assess bone density and anatomy.
-
Diagnostic wax-up: Creating a model of what your final smile will look like.
-
Surgical guide fabrication: Often using 3D printing to ensure precise implant placement.
During this phase, your dentist determines the ideal positions for the implants. If you are missing three teeth, they will decide whether to place two implants or three. The decision to use a pontic often comes down to bone availability, financial considerations, and long-term prognosis.
Phase 2: Surgical Placement
The first surgical code you will see is typically D6010, which covers the placement of the implant body into the jawbone. For a three-unit bridge requiring two implants, you will see this code twice.
After placement, a healing period of three to six months usually follows. This allows the implant to fuse with the bone—a process known as osseointegration.
Phase 3: Abutment Connection
Once the implants have integrated, your dentist will uncover them and place the abutments. An abutment is the piece that connects the implant to the final restoration. The code used here is often D6056 (prefabricated abutment) or D6057 (custom abutment). Custom abutments are typically more expensive but offer better aesthetics if the implant is in a visible area.
Phase 4: Impression and Fabrication
This is where D6064 enters the picture. After the abutments are placed, your dentist takes a highly precise impression of the abutments and the surrounding soft tissue. This impression is sent to a dental laboratory.
The lab technician will fabricate the bridge. This structure includes:
-
Crowns that will fit over the abutments.
-
One or more pontics that will fill the gaps between the crowns.
The pontic is designed to look exactly like a natural tooth. It must also be shaped to allow for proper hygiene, as cleaning under a pontic is different from cleaning a natural tooth.
Phase 5: Delivery and Adjustment
When the restoration returns from the lab, you will return to the office for the delivery appointment. The dentist will check the fit, the bite, and the color match. Adjustments are made to ensure the pontic does not place undue stress on the supporting implants. The restoration is then cemented or screwed into place.
At this point, D6064 is finalized as a completed service.
Cost Considerations for D6064
One of the most common questions patients ask is, “How much does an implant pontic cost?”
The answer is rarely straightforward because D6064 is almost never billed in isolation. However, understanding the variables that influence the cost of this code can help you budget effectively.
Factors That Influence Price
-
Geographic Location: Dental fees vary significantly between urban and rural areas, as well as between regions.
-
Laboratory Fees: High-quality materials such as monolithic zirconia or layered porcelain cost more to fabricate.
-
Dentist Expertise: Prosthodontists or oral surgeons may charge higher fees for complex cases involving implant pontics.
-
Material Choice: A porcelain-fused-to-metal (PFM) pontic is generally less expensive than a full-zirconia or all-ceramic pontic.
-
Custom Abutments: If the pontic is part of a larger restoration using custom abutments (D6057), the overall lab bill increases.
Average Fee Ranges
While exact prices vary, here is a general estimate of what you might expect to see on a treatment plan for the restorative phase (the part involving D6064):
| Procedure | Code | Estimated Fee Range (USD) |
|---|---|---|
| Implant Abutment (Prefabricated) | D6056 | $400 – $800 per abutment |
| Implant Abutment (Custom) | D6057 | $800 – $1,500 per abutment |
| Abutment Supported Crown | D6062 | $1,200 – $2,500 per crown |
| Abutment Supported Pontic | D6064 | $1,100 – $2,200 per pontic |
These fees are for the restorative components only. The surgical placement of the implants (D6010) is billed separately and typically ranges from $1,500 to $3,000 per implant.
Insurance and D6064: What You Need to Know
Navigating dental insurance for implant procedures can be frustrating. Many patients assume that because they have dental insurance, most of the cost will be covered. Unfortunately, this is often not the case with implants.
Why Implants Are Often a “Gray Area”
Traditional dental insurance plans were designed decades ago to cover preventive care and basic restorations like fillings and tooth-supported bridges. Implants are still considered a “major” service, and many plans have specific exclusions for them.
When it comes to D6064, here are the typical insurance scenarios:
-
No Implant Coverage: Many PPO plans explicitly exclude implants. In this case, D6064 is considered a non-covered service, and the patient is responsible for the full fee.
-
Alternative Benefit Clause: Some plans offer an “alternative benefit.” If your plan covers a traditional tooth-supported bridge (e.g., D6245) but not implants, the insurance may pay what they would have paid for the traditional bridge and apply that amount toward the implant pontic.
-
Waiting Periods: For major services, many plans have a 6 to 12-month waiting period. If you are new to the plan, you may have to wait before D6064 is eligible.
-
Annual Maximums: Most dental plans have an annual maximum (usually between $1,000 and $2,000). Since a full implant case often costs well over $10,000, the insurance will only cover a fraction of the total.
How to Verify Coverage
To avoid surprises, take these steps before treatment begins:
-
Request a Pre-treatment Estimate: Ask your dentist to send a pre-authorization to your insurance company. This is a formal estimate of what will be paid for codes like D6064.
-
Understand Your Policy Language: Look for terms like “implant restoration,” “prosthetic abutment,” and “fixed partial denture.” These will clue you in on how D6064 is categorized.
-
Ask About Dual Coverage: If you have coverage through a spouse or a secondary plan, you may be able to maximize benefits across both.
The Difference Between a Pontic and a Crown in Implant Dentistry
A frequent point of confusion lies in distinguishing between a pontic and a crown when implants are involved. While they look similar in the mouth, the codes, function, and billing are distinct.
Abutment Supported Crown (D6062)
This code is used for a crown that is cemented or screwed onto an abutment that is attached to an implant. This crown has its own dedicated implant beneath it. It bears the full force of biting and chewing directly on that implant.
Abutment Supported Pontic (D6064)
This code is used for an artificial tooth that does not have its own implant. It is suspended between two abutments. The forces of biting are transferred through the pontic to the adjacent abutments and then to the implants beneath them.
Why the Distinction Matters for Your Treatment
From a clinical perspective, this distinction matters because the biomechanics are different. A pontic must be designed to minimize stress on the supporting implants. If a pontic is placed in a high-stress area (like the molar region) without adequate support, the risk of mechanical failure increases.
From a financial perspective, knowing which teeth are pontics and which are crowns helps you verify that you are being billed correctly. If you are receiving a three-unit bridge with two implants, you should expect to see two D6062 codes (for the crowns over the implants) and one D6064 code (for the pontic in the middle).
Material Choices for Implant Pontics
When your dentist bills D6064, the material used to fabricate the pontic is a key factor in the final cost and appearance. Today, patients have more options than ever before.
Porcelain-Fused-to-Metal (PFM)
This is the traditional choice. A metal substructure provides strength, while porcelain is layered over it to mimic the appearance of a natural tooth.
-
Pros: Durable, time-tested, generally less expensive.
-
Cons: Over time, the gum line may recede, revealing a dark metal margin. The porcelain can also chip.
Full Zirconia
Zirconia is a high-strength ceramic that is often used for posterior (back) teeth. It is incredibly strong and resistant to fracture.
-
Pros: Extremely durable, biocompatible, no metal.
-
Cons: Can be abrasive to opposing teeth if not polished correctly. It may not have the translucency of natural teeth.
Lithium Disilicate (e.g., E.max)
This is a glass-ceramic material known for its superior aesthetics. It is often the material of choice for anterior (front) pontics where appearance is paramount.
-
Pros: Exceptional aesthetics, excellent translucency, biocompatible.
-
Cons: Slightly less fracture-resistant than zirconia, making it less ideal for heavy grinding cases.
High-Noble Metal
In some cases, particularly for patients with heavy bruxism (teeth grinding), a full gold or high-noble metal pontic may be recommended. While not aesthetically ideal for visible areas, it is the most biocompatible and least abrasive material available.
Important Note: The material used is often not specified in the code D6064 itself. However, it should be clearly listed in your treatment plan description. If you have preferences or concerns about allergies (such as nickel sensitivity), discuss these with your dentist before the restoration is fabricated.
Common Clinical Scenarios for D6064
To help you visualize how this code applies in real-world situations, let us explore a few patient cases.
Scenario 1: The Three-Unit Anterior Bridge
Patient Profile: A 45-year-old patient missing the upper right lateral incisor (tooth #7) and central incisor (#8). Bone volume is insufficient for two implants in the front, but sufficient for one implant in the #7 position and one implant in the #9 position.
Treatment Plan:
-
Two implants placed (D6010 x 2).
-
Two custom abutments (D6057 x 2).
-
A three-unit restoration: Crown on #7 (D6062), crown on #9 (D6062), and a pontic replacing #8 (D6064).
Outcome: The pontic (D6064) fills the gap seamlessly, giving the illusion of three independent teeth while utilizing only two implants.
Scenario 2: The Five-Unit Posterior Bridge
Patient Profile: A 60-year-old patient missing teeth #18, #19, #20, and #21. The patient wishes to avoid a removable partial denture but wants to minimize the number of implants due to cost.
Treatment Plan:
-
Two implants placed at the distal (far back) and mesial (front) ends of the edentulous space.
-
Two custom abutments.
-
A five-unit restoration: Two crowns (D6062) over the implants, and three pontics (D6064 x 3) in between.
Outcome: This is an efficient use of implants. However, the patient is cautioned that the long span of pontics requires meticulous hygiene to prevent peri-implant disease.
Scenario 3: Implant to Natural Tooth
Patient Profile: A 35-year-old patient missing tooth #4. Tooth #3 is healthy and strong. The patient does not want a removable partial, and placing an implant adjacent to #3 is complicated due to sinus proximity.
Treatment Plan:
-
One implant placed in the #4 position.
-
A custom abutment on the implant.
-
A three-unit bridge: Crown on natural tooth #3, pontic on #4 (D6064), and crown on implant #5 (D6062).
Outcome: This approach is controversial among dentists because natural teeth have slight mobility (periodontal ligament), while implants are rigid (ankylosed). Over time, the difference in movement can cause issues. Many modern dentists prefer to avoid this configuration unless the natural tooth can be “non-rigidly” connected. If you see this in your treatment plan, ask your dentist about long-term prognosis.
Maintenance and Longevity of an Implant Pontic
Once your implant pontic is placed, the work is not over. In fact, the long-term success of the restoration depends heavily on how you maintain it.
Hygiene Challenges
A pontic does not have a natural tooth root, so there is no periodontal ligament. This means there is no natural defense mechanism against bacteria. The space under the pontic—where it meets the gum tissue—can trap food and plaque.
To maintain health:
-
Use Superfloss or Interdental Brushes: You must clean underneath the pontic daily. Regular floss cannot do this effectively.
-
Water Flossers: A water flosser can be a game-changer for flushing out debris from under the pontic.
-
Professional Maintenance: Your dentist or hygienist will need to check the abutment screws (if screw-retained) and assess the health of the gum tissue around the implants. This is typically done during your regular six-month cleanings.
Expected Lifespan
With proper care, a high-quality implant-supported bridge (including the pontic) can last 15 to 20 years or more. However, several factors influence longevity:
-
Oral Hygiene: The most critical factor. Peri-implantitis (inflammation around the implant) is the leading cause of implant failure.
-
Parafunctional Habits: If you grind or clench your teeth, the pontic and supporting implants are subjected to excessive forces. A nightguard may be necessary.
-
Material Quality: Higher-grade ceramics and well-fabricated restorations tend to have fewer issues with chipping or fracture.
-
Biomechanical Design: A pontic that is too long (spanning multiple missing teeth) places more stress on the supporting implants.
Alternatives to an Implant Pontic
While D6064 is an excellent solution for many patients, it is not the only path forward. Depending on your clinical situation, budget, and preferences, you might consider these alternatives.
1. Single Implant Crowns for Each Missing Tooth
Instead of using pontics, you could place an implant for every missing tooth. Each would be restored with a single crown (D6062).
-
Pros: Easier hygiene (each implant is independent), no risk of pontic fracture, biomechanically simpler.
-
Cons: Significantly higher cost. More surgical procedures. Longer treatment time.
2. Traditional Tooth-Supported Fixed Bridge
If you have healthy teeth adjacent to the gap, you could opt for a traditional bridge. This uses the natural teeth as abutments.
-
Pros: Lower upfront cost. Faster completion (no waiting for osseointegration). Usually covered by insurance.
-
Cons: Requires drilling down healthy tooth structure. Does not prevent bone loss in the edentulous area. Shorter lifespan than implants.
3. Removable Partial Denture
A cast metal or flexible partial denture can replace missing teeth without any surgery.
-
Pros: Most affordable option. No surgery. Easily repairable.
-
Cons: Less stable. Can be uncomfortable. Accelerates bone loss over time. Patients often find them inconvenient.
4. Resin-Bonded Bridge (Maryland Bridge)
This is a conservative option often used for missing front teeth. It involves a pontic with “wings” that are bonded to the back of adjacent teeth.
-
Pros: Minimal preparation of adjacent teeth. Lower cost.
-
Cons: Not suitable for high-bite-force areas. Can debond over time.
Comparison Table: Implant Pontic vs. Alternatives
| Feature | Implant Pontic (D6064) | Single Implant Crowns | Traditional Bridge | Removable Partial |
|---|---|---|---|---|
| Surgery Required | Yes | Yes | No | No |
| Affects Adjacent Teeth | No | No | Yes | Minimal |
| Prevents Bone Loss | Yes | Yes | No | No |
| Typical Cost | High | Very High | Moderate | Low |
| Longevity | 15-20+ years | 20+ years | 10-15 years | 5-10 years |
| Hygiene Ease | Moderate | Easy | Difficult | Moderate |
The Importance of Accurate Coding for Patients
You might wonder why, as a patient, you need to understand the dental code for an implant pontic. The answer lies in accountability and transparency.
Mistakes in dental coding can happen. In some cases, a dentist’s billing department might inadvertently use the wrong code, which could lead to:
-
Insurance Denials: If D6064 is used when D6062 should have been used, the claim may be rejected.
-
Unexpected Costs: If a code is not covered under your plan but a similar code is, you could end up paying more out of pocket.
-
Inaccurate Records: Your dental records should accurately reflect the treatment you received for future reference.
By familiarizing yourself with D6064, you can review your treatment plan and ask clarifying questions. For instance, you can ask:
-
“Why is this pontic billed under D6064 rather than a traditional bridge code?”
-
“Are the supporting abutments included in this fee, or will they be billed separately?”
-
“What material is being used for the pontic, and is that specified in the code?”
Future Trends in Implant Pontic Coding
The world of dental coding is not static. The CDT manual is updated annually, and changes often reflect advances in technology and clinical practice.
Digital Dentistry Integration
As intraoral scanners and CAD/CAM (computer-aided design and computer-aided manufacturing) become the standard, the line between laboratory fees and clinical fees is blurring. Some offices now offer same-day milling of implant bridges, including pontics, using advanced systems.
While the code D6064 remains the same, the delivery method is evolving. In the future, we may see separate codes for digitally fabricated pontics versus conventionally fabricated ones, similar to what happened with crowns (D2740 vs. D2750 for CAD/CAM).
Screw-Retained vs. Cemented Pontics
There is a growing trend toward screw-retained implant bridges. In this design, the entire bridge (including pontics) is fabricated as a single piece and screwed directly onto the implants. This eliminates the need for cement, which can sometimes cause peri-implant inflammation.
In a screw-retained bridge, the pontic is still coded as D6064, but the abutment codes (D6056/D6057) may not be used because the abutment and restoration are integrated. Understanding this can help you see why some treatment plans look different from others.
Frequently Asked Questions (FAQ)
1. Is D6064 covered by dental insurance?
It depends on your specific plan. Many dental insurance plans exclude implants entirely. However, some plans offer an “alternative benefit” where they pay the equivalent of a traditional bridge. Always request a pre-treatment estimate to know your out-of-pocket cost.
2. Does D6064 include the cost of the implant itself?
No. D6064 covers only the pontic (the artificial tooth) and its placement onto the abutment. The implant body is billed under D6010, and the abutment is billed under D6056 or D6057.
3. How long does it take to get an implant pontic?
The entire process—from implant placement to final restoration—typically takes 4 to 9 months. This allows time for osseointegration (healing of the implant to the bone) before the pontic is fabricated and placed.
4. Can an implant pontic be replaced if it breaks?
Yes. If the pontic fractures, it can be replaced without removing the implants. However, the replacement process involves sending the abutments back to the lab to fabricate a new bridge. This will incur additional laboratory and clinical fees.
5. Is an implant pontic painful to place?
The placement of the pontic itself is not painful because it occurs after the implants have healed. You will be under local anesthesia during the delivery appointment to ensure comfort. Post-procedure sensitivity is usually minimal.
6. What is the difference between D6064 and D6245?
D6245 is a code for a pontic that is part of a traditional tooth-supported fixed bridge. D6064 is for a pontic that is supported by dental implant abutments. The difference is the supporting structure.
Additional Resources
For those who wish to dive deeper into the technical aspects of dental coding and implant prosthetics, the following resources are invaluable:
-
American Dental Association (ADA) CDT Code Book: This is the official manual used by dentists across the United States. You can purchase the current edition directly from the ADA website to review the exact descriptors for all implant codes.
-
American Academy of Implant Dentistry (AAID): This organization provides patient education materials and can help you find qualified implant dentists in your area.
Link: https://www.ada.org/en/publications/cdt
Conclusion
Understanding the dental code for an implant pontic—D6064—empowers you to take control of your dental treatment. This code represents more than just a billing number; it represents a sophisticated restoration that combines surgical precision with artistic craftsmanship to replace missing teeth.
We have explored what a pontic is, the specific clinical scenarios that require D6064, the costs involved, and how insurance typically handles implant restorations. We also discussed the importance of material choices, the differences between pontics and crowns, and the long-term maintenance required to ensure your investment lasts for decades.
Armed with this knowledge, you can now approach your dental consultation with confidence. You know the right questions to ask, you understand how to read your treatment plan, and you are prepared to make informed decisions about your oral health.
Disclaimer Reiteration: This content is for educational purposes only. Dental coding and insurance policies are subject to change. Please consult your dental provider for a personalized treatment plan and accurate cost estimates.
Disclaimer: This article is for informational purposes only and does not constitute medical, financial, or legal advice. Dental coding practices vary by region and insurance provider. Always consult with your dental provider and insurance carrier for specific billing inquiries.
Author: Professional Technical Writer Team
Date: March 24, 2026





