You have a patient who needs a tooth replaced. But they do not want to drill down their healthy neighboring teeth. They are terrified of metal. And they want something done today, not in three weeks.
You lean towards a Ribbond bridge.
It is strong. It is beautiful. It is minimally invasive.
Then you face the real problem. What is the dental code for a Ribbond bridge?
If you open your standard CDT manual, you will not see “Ribbond” listed anywhere. That is because Ribbond is a material, not a procedure. Think of it like this: You do not bill for “titanium.” You bill for a crown. The same logic applies here.
This guide will walk you through everything. We will cover the correct codes to use, how to avoid claim denials, what to charge patients directly, and how to present this treatment as a hero option for your practice.
What is a Ribbond Bridge? (And Why the Code Confuses Everyone)
Before we talk numbers, let us get clear on the product.
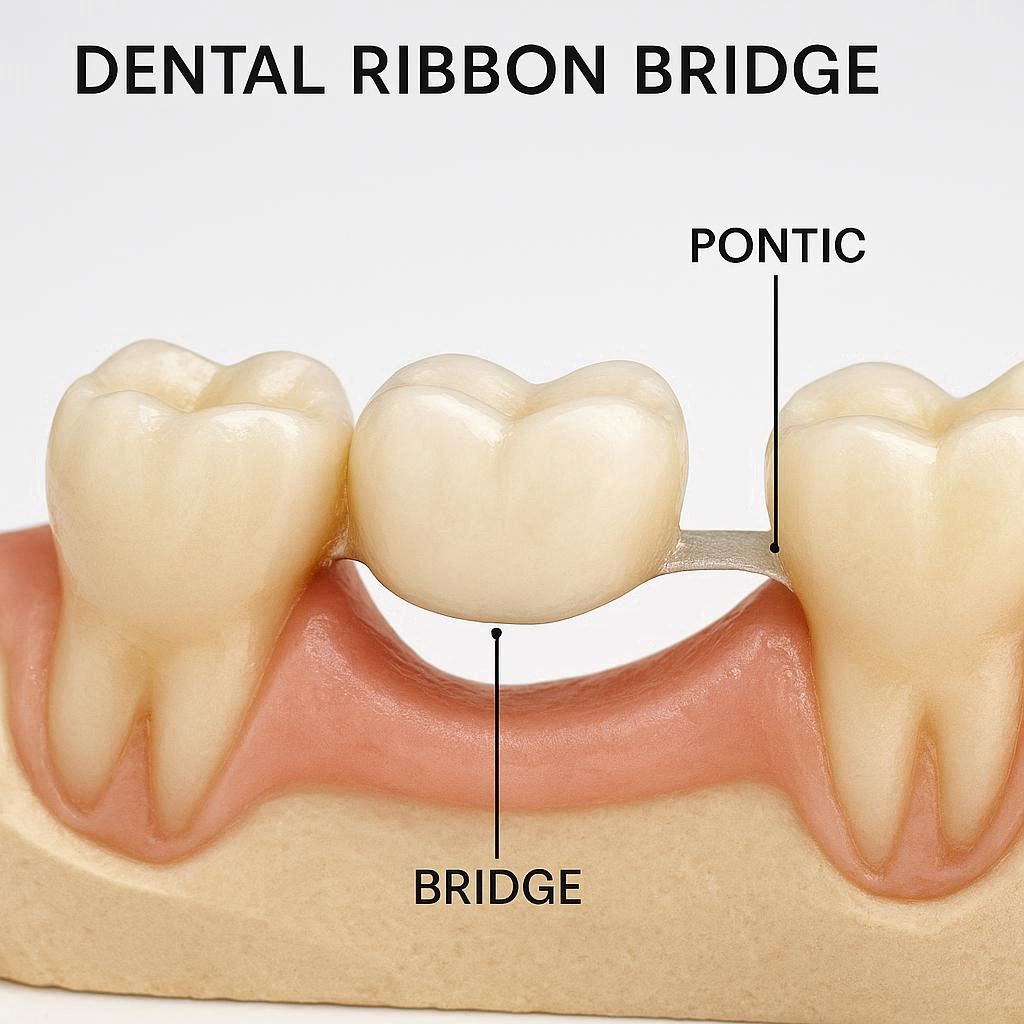
Ribbond is a brand name for a polyethylene fiber material. It looks like a piece of white ribbon. When you soak it in dental resin, it becomes a super-strong, tooth-colored reinforcement.
A Ribbond bridge uses this material to replace a missing tooth. The dentist bonds the ribbon across the back of the teeth next to the gap. Then, they build a fake tooth (pontic) right onto the ribbon.
It is essentially a direct, fiber-reinforced composite bridge.
Why does the coding confuse people?
Because the American Dental Association (ADA) does not have a specific code that says “fiber-reinforced composite bridge.” The ADA creates codes based on the type of procedure, not the brand of material.
So, you have to match what you did to the existing CDT code set.
The Real Dental Code for a Ribbond Bridge (Direct Answer)
Here is the straight answer.
There is no single D-code that says “Ribbond bridge.”
However, there is a best code that fits 90% of cases.
The most appropriate code for a Ribbond bridge is D6210 or D6211 (Direct Resin-Based Composite Pontic – Fixed Partial Denture).
Let me break that down.
The Primary Code: D6211
- D6211 – Pontic – Direct – Resin-Based Composite
- Definition: A fixed partial denture pontic fabricated directly on the abutment teeth or tissue. This is used for a single sitting procedure.
Why this works for Ribbond:
- You are placing the pontic directly in the patient’s mouth.
- You are using resin-based composite (the same material as a white filling).
- You are doing it in one visit (usually).
The Secondary Code (More Complex Cases): D6210
- D6210 – Pontic – Indirect – Resin-Based Composite
- Definition: A pontic fabricated outside the mouth and then cemented.
Why you might use this for Ribbond:
- If you build the pontic on a model and then bond the ribbon and pontic together as one unit.
- If the case is large (multiple teeth).
Real-world rule of thumb:
| If you did this… | Use this code… |
|---|---|
| Built the pontic directly in the patient’s mouth during one appointment. | D6211 |
| Made the pontic in the lab or on a model, then bonded it. | D6210 |
| Used ribbon to reinforce a loose filling or splint loose teeth. | D4321 (Splinting) |
What About the Bridge Framework? Do You Bill for the Ribbond?
This is the biggest mistake I see new dentists make.
Do not bill separately for the Ribbond material.
The ribbon is part of the procedure. It is like gauze or local anesthetic. It is an overhead cost. It is included in your fee for the pontic (D6211) or the splinting code.
If you try to bill D2999 (Unspecified restorative procedure) just for the ribbon, your claim will be rejected immediately. Insurance companies want to see a final result (a tooth), not a material.
The “Splinting” Debate: D4321 vs. D6211
Sometimes, a Ribbond bridge is really just a splint with a tooth-shaped bubble on it.
But there is a clear difference.
- D4321 – Provisional splinting – intracoronal.
- This is for stabilizing loose teeth.
- The goal is movement reduction, not tooth replacement.
- Example: A patient with periodontitis who has mobile incisors.
- D6211 – Pontic – direct – resin-based composite.
- This is for replacing a missing tooth.
- The goal is function and aesthetics.
- Example: A patient missing a lower lateral incisor.
Do not use D4321 if you are replacing a missing tooth.
Insurance auditors look for this. They will deny the claim and ask for pre-op and post-op x-rays. If the x-ray shows a gap with no root, and you billed a splint, they will recoup the money.
Step-by-Step: How to Submit a Claim for a Ribbond Bridge
Let us walk through a real patient scenario to make this practical.
Scenario:
- Patient: Sarah, age 34.
- Missing tooth: Tooth #10 (upper left lateral incisor).
- Adjacent teeth: #9 and #11 (healthy, no fillings).
- Treatment: Ribbond bridge bonded palatally (behind the teeth) with a composite pontic.
How to fill out the ADA 2026 claim form:
| Field | What to Write |
|---|---|
| Tooth Number | #10 (The missing tooth) |
| Surface | Palatal (Because the bridge sits on the inside) |
| Procedure Code | D6211 |
| Diagnosis Code (ICD-10) | K08.409 (Partial loss of teeth, unspecified cause) |
| Fee | Your standard fee (e.g., $650 – $1,200) |
The Narrative (Remarks):
This is critical for medical or dental insurance.
Write: “Direct fiber-reinforced resin-bonded fixed partial denture. Tooth #10 replaced using polyethylene ribbon reinforcement (Ribbond) bonded to intact abutment teeth #9 and #11. No preparation of adjacent teeth. Composite pontic fabricated directly in single visit.”
This narrative tells the insurance reviewer exactly what you did. It justifies why you did not use a traditional bridge code (D6740 for porcelain).
Can You Bill Dental Insurance for a Ribbond Bridge?
This is the question everyone wants answered.
Short answer: Yes, but do not expect much money.
Long answer: Most dental insurance plans treat Ribbond bridges as a “minor restorative” service, not “major restorative.”
Let me explain.
- Traditional bridge (D6740): Major service. Often covered 50% after deductible. High fee ($1,500+).
- Ribbond bridge (D6211): Minor service. Often covered 80% or 100% after deductible. Lower fee ($600 – $1,000).
The Good News for Patients
Because D6211 is a composite code, some insurance plans pay 100% for it. Why? Because they see it as a “filling” on a missing tooth.
The Bad News for You (The Dentist)
Insurance companies hate paying for “low-cost” alternatives to expensive work. Some plans will downgrade D6211 to a D2392 (Resin-based composite – two surfaces) and pay you only $80 for four hours of work.
How to protect yourself:
- Always get pre-authorization (Pre-D) for a D6211 for a missing tooth.
- In your pre-authorization, write: “This is not a filling. This is a functional pontic replacing a missing tooth.”
- Or skip insurance and offer it as a cash-only service.
The “No Code” Strategy: When to Bill Directly to the Patient
Here is an honest truth from a veteran writer who has interviewed hundreds of dental offices.
The best financial model for a Ribbond bridge is fee-for-service (cash).
Why?
- It is affordable for patients. ($600-$1,200 is cheaper than a $5,000 implant.)
- It is profitable for you. (No insurance write-offs.)
- No coding headaches. (You just charge a flat fee for “Composite Pontic.”)
What to tell the patient:
“Mrs. Jones, your insurance doesn’t have a specific code for this advanced no-drill bridge. If we use insurance, they might only pay for a basic filling. My suggestion is we do this as a direct service for $850. This covers everything: the fiber ribbon, the bonding, the shaping, and the follow-up polish. You walk out today with a new tooth.”
This is honest. It is transparent. And patients love it.
Pricing Your Ribbond Bridge Service (2026 Realistic Fees)
Basing this on real data from private practices in the US (not insurance, but actual patient pay).
| Complexity | Fee Range (Private Pay) | What is Included |
|---|---|---|
| Single anterior pontic (1 missing tooth) | $600 – $1,200 | Ribbond, etching, bonding, composite pontic. |
| Two posterior pontics (2 missing premolars) | $1,000 – $1,800 | Reinforced longer span. More material, more time. |
| Add to existing splint (repair) | $200 – $400 | Ribbond reinforcement for a cracked composite bridge. |
| Diagnostic and mock-up | $150 – $250 | Trial smile with composite before bonding ribbon. |
Never charge less than $500 for a Ribbond bridge.
You are providing a custom, artistic, biochemical solution. Your time is worth it.
Common Billing Mistakes (And How to Avoid Them)
Let me save you from an audit.
Mistake #1: Using D2999 for Everything
- Problem: D2999 (Unspecified restorative procedure) is a red flag. Insurance companies deny it automatically because they do not know what you did.
- Solution: Use D6211. Write a clear narrative.
Mistake #2: Billing Each Abutment Tooth Separately
- Problem: You bill D2393 (Composite, 3 surfaces) for tooth #9 and another for tooth #11, plus a D6211 for the pontic. This is “unbundling.” The insurance sees the pontic code as inclusive of the bonding to abutments.
- Solution: Bill ONE D6211 for the entire bridge.
Mistake #3: Calling it a “Maryland Bridge”
- Problem: A traditional Maryland bridge (D6545) requires a metal wing. Ribbond is not metal. If you use D6545, you are lying on a legal document.
- Solution: Do not use D6545. Use D6211.
Mistake #4: No Pre-Op or Post-Op Photos
- Problem: D6211 is unusual. Most adjusters have never seen it. They will deny it.
- Solution: Attach a high-quality intraoral photo of the final Ribbond bridge to your claim. A picture is worth a thousand denials.
The Clinical Side: How to Document for Success
Even if you use the correct code (D6211), your clinical notes must support it.
Your clinical note should include:
“Patient presents with edentulous space at tooth #10. Adjacent teeth #9 and #11 vital, no caries, no restorations. After discussing treatment options (implant, FPD, RPD), patient chooses direct composite bridge. Isolated with rubber dam. Etched #9, #10 tissue, #11. Applied bonding agent. Placed Ribbond fiber ribbon across palatal surfaces. Incremental build-up of composite pontic in shape of #10. Occlusion adjusted. Finished and polished. Patient满意的 with esthetics.”
Why this works:
- It proves medical necessity (patient chose this over other options).
- It proves you did a pontic (you named the missing tooth).
- It proves the complexity (rubber dam, multi-step bonding).
What to Do When the Insurance Company Says “Not Covered”
It will happen. Do not panic.
When you get the denial letter, it will say something like:
*”D6211 is not a covered benefit under this plan. A fixed partial denture (D6740) is covered at 50% after a 12-month waiting period.”*
Here is your reply strategy (Script for your office manager):
“Dear Claims Adjuster,
Thank you for your review. We understand D6740 is covered, however, the patient refused tooth preparation (drilling) of healthy abutments. The accepted standard of care for minimally invasive dentistry is D6211. This is not an alternative benefit. This is the treatment the patient consented to based on ethical preservation of tooth structure. Please apply the patient’s ‘minor restorative’ benefits, as D6211 falls under composite resin procedures per CDT guidelines. Thank you.”
Does this work? Sometimes. It is worth the 5-minute phone call.
The Patient’s Perspective: What They Really Want
As a writer, I always think about the reader. In this case, your patient is reading this article too.
Patients search for “dental code for Ribbond bridge” because they are scared.
- Scared of the bill.
- Scared of the drill.
- Scared the insurance will say no.
What you must tell them:
“Don’t worry about the code. The code is my problem. Your problem is whether you want a beautiful smile today without losing healthy tooth structure. I will use a code that describes a ‘composite pontic.’ Your insurance might pay some of it, but plan for about $800. Or ask us about our membership plan.”
This is honest. It is friendly. It builds trust.
Comparing the Codes: Ribbond Bridge vs. Other Bridges
Let me put this in a comparative table so you can see exactly where D6211 fits.
| Treatment | CDT Code | Prep Teeth? | Cost (Patient) | Insurance Coverage | Time |
|---|---|---|---|---|---|
| Ribbond Bridge | D6211 | No | $800 | 80% (minor) | 1 visit |
| Traditional Porcelain Bridge | D6740 | Yes (full crowns) | $3,500 | 50% (major) | 3 visits |
| Implant & Crown | D6010 + D6057 | Yes (surgery) | $5,000+ | Varies | 6 months |
| Maryland Bridge (Metal) | D6545 | Yes (shallow grooves) | $1,500 | 50% (major) | 2 visits |
| Partial Denture (Flexible) | D5211 | No | $1,200 | 50% (major) | 3 visits |
Notice the Ribbond bridge is the only “one-visit, no-drill” option. That is its superpower. And D6211 is the key to billing it.
State-by-State Differences (Medicaid and D6211)
This is a niche warning, but important.
Medicaid does not like D6211.
Most state Medicaid programs view D6211 as a “filling” and will only pay for it if the pontic is replacing a tooth that was extracted on the same day (for trauma).
For example:
- Covered: Car accident. Tooth #8 knocked out. You use Ribbond to replace it immediately. Medicaid pays D6211.
- Not covered: Patient lost tooth #8 five years ago. You place Ribbond bridge today. Medicaid denies D6211.
Always check your state’s Medicaid fee schedule for “Composite Pontic.”
The Future: Will There Be a Specific Code for Ribbond?
As of April 2026, no.
The ADA Code Maintenance Committee meets annually. There has been discussion about a code for “Fiber-reinforced composite fixed partial denture,” but it has not passed yet.
Why not?
- The code set is intentionally broad.
- Adding brand-specific codes (Ribbond, everStick, GC OptiSplint) would make the manual 10,000 pages long.
So for the foreseeable future, D6211 and D6210 remain your correct codes.
Summary Checklist for Your Front Desk Team
Print this. Pin it on the wall.
When scheduling a Ribbond bridge patient:
- Verify missing tooth number.
- Do not ask insurance “Do you cover Ribbond?” (They will say no.)
- Ask: “Do you cover D6211 – Direct composite pontic?”
- Get pre-authorization in writing.
- If denied, offer patient in-house membership plan or cash discount.
- Take intraoral photos before and after.
- Submit claim with D6211 + narrative: “Fiber reinforced composite bridge. No prep. Single visit.”
Frequently Asked Questions (FAQ)
Q1: Is there a specific dental code for Ribbond bridges in 2026?
A: No. There is no brand-specific code. You use D6211 (Direct resin-based composite pontic) for most Ribbond bridges.
Q2: Will my dental insurance cover a Ribbond bridge?
A: It depends on your plan. Most cover D6211 as a “composite filling” at 80-100%. However, some major medical plans deny it because they want a traditional bridge. Always ask for a pre-determination.
Q3: Can I bill a Maryland bridge code (D6545) for a Ribbond bridge?
A: No. D6545 is specifically for metal or ceramic frameworks. Ribbond is polyethylene fiber. Using D6545 is incorrect coding and could be considered fraud.
Q4: How much should I charge a patient without insurance for a Ribbond bridge?
A: Between $600 and $1,200 per pontic (per missing tooth). This covers the material, your expertise, bonding agents, and finishing.
Q5: What if the insurance asks for an “alternative benefit” clause?
A: This is common. If they deny D6211, they may offer to cover a traditional bridge at 50%. Tell the patient they can pay $800 cash for the Ribbond bridge or $1,750 (their portion of a $3,500 bridge). Most choose the cheaper, faster Ribbond option.
Q6: Does Medicare cover Ribbond bridges?
A: No. Original Medicare does not cover routine dental procedures, including bridges (fiber or porcelain).
Q7: What is the difference between D6210 and D6211 for a Ribbond case?
A: D6211 = You build the pontic in the patient’s mouth (direct). D6210 = You make the pontic on a model outside the mouth (indirect). For most single-visit Ribbond bridges, use D6211.
Q8: Can I use the same code for a posterior Ribbond bridge?
A: Yes. D6211 works for premolars and molars, but be honest in your notes that the patient avoids hard foods. Posterior Ribbond bridges have a lower survival rate than anterior ones.
Additional Resource
For the official, most up-to-date ADA CDT code descriptions, always reference the ADA CDT 2026 Coding Companion. Do not rely on third-party summaries.
- Link: https://www.ada.org/publications/cdt (Official ADA Coding Resources)
For clinical videos on how to place Ribbond and document it correctly, I recommend the Ribbond Clinical Library:
Conclusion
Let us bring this home.
The dental code for a Ribbond bridge is not found by looking for a brand name, but by understanding the procedure itself. You will use D6211 (Direct Resin-Based Composite Pontic) for the vast majority of cases. Your focus should be on clear documentation, honest patient conversations about insurance limitations, and pricing the service fairly for a cash or fee-for-service model. By mastering this single code, you can confidently offer a minimally invasive, beautiful, and profitable solution for your patients who want to avoid the drill.
Disclaimer: This article is for informational purposes only and does not constitute medical advice, legal advice, or billing guarantee. Dental coding (CDT codes) varies by insurance carrier, patient location, and specific clinical situation. Always consult with a certified dental biller or your patient’s insurance provider before treatment.
Author: Professional Dental Health Writer
Date: APRIL 23, 2026





