If you are an anesthesiologist, certified registered nurse anesthetist (CRNA), or a medical biller, you have likely encountered the acronym “IPACK.” The IPACK block (Infiltration of the Popliteal Artery and Capsular Knee) is a fantastic, modern pain management technique for total knee arthroplasty (TKA) and other knee surgeries. It provides excellent posterior knee analgesia without causing the motor weakness associated with a sciatic nerve block.
However, when it comes time to bill for this service, a major problem arises: There is no specific CPT code for an IPACK block.
That single sentence frustrates many professionals. But do not worry. This guide will walk you through every available option, from unlisted codes to peripheral nerve block codes, so you can bill accurately, remain compliant, and maximize your reimbursement.
Let us dive into the realistic world of IPACK block coding.
CPT Code for IPACK Block
Table of Contents
ToggleWhat Exactly is an IPACK Block?
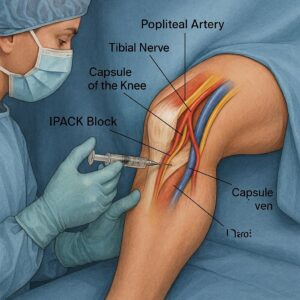
Before we discuss numbers, let us ensure we understand the procedure. The IPACK block is an ultrasound-guided injection of local anesthetic into the space between the popliteal artery and the posterior capsule of the knee.
Its primary goal is to block the terminal branches of the genicular nerves (specifically the posterior articular branches of the tibial and obturator nerves) that supply the posterior knee joint. Because the local anesthetic is deposited around the artery and capsule—not near the main nerve trunks—the patient retains quadriceps and foot dorsiflexion strength. This allows for early ambulation after knee replacement surgery.
Common Surgeries Associated with IPACK:
-
Total knee arthroplasty (TKA)
-
Unicompartmental knee arthroplasty
-
Anterior cruciate ligament (ACL) reconstruction (in some protocols)
-
Knee osteotomy
Why the Confusion?
The American Medical Association (AMA) and the Current Procedural Terminology (CPT) code set are constantly evolving. New procedures often take years to receive a unique code. As of 2026, the IPACK block remains a relatively new technique, so no dedicated code exists. You must “map” the procedure to the closest existing code or use an unlisted code.
The Main Coding Options for IPACK Block
When you search for the “cpt code for ipack block,” you will find three primary pathways. Each has pros, cons, and specific documentation requirements. No single answer fits every payer.
| Coding Option | CPT Code | Description | Best Use Case |
|---|---|---|---|
| Unlisted Code | 64999 | Unlisted procedure, nervous system | Initial attempt for commercial payers; when no other code applies |
| Peripheral Nerve Block | 64447 | Injection, anesthetic agent; femoral nerve | Incorrect – do not use for IPACK |
| Peripheral Nerve Block | 64448 | Injection, anesthetic agent; sciatic nerve | Incorrect – do not use for IPACK |
| Somatic Nerve Block | 64450 | Injection, anesthetic agent; other peripheral nerve or branch | Controversial – some coders use, but risk of audit |
| Chemical Denervation | 64632 | Destruction by neurolytic agent; genicular nerve branch | Incorrect – not for temporary surgical blocks |
Let us break down the two viable options: 64450 (with caution) and 64999 (the safest approach).
Option 1: CPT 64999 – Unlisted Procedure, Nervous System
This is often the most defensible code for an IPACK block. Because the IPACK block targets a specific anatomic space (between the popliteal artery and the posterior capsule) rather than a named peripheral nerve, it does not fit neatly into codes like 64450 (which requires a named nerve).
When to use 64999:
-
For almost all commercial insurance plans (UnitedHealthcare, Cigna, Aetna, etc.).
-
When your medical director advises against “forcing” the block into a defined nerve code.
-
When you want to be as accurate as possible to the procedure description.
The challenge with 64999: Payers hate unlisted codes. They often require paper claims, medical records, and a cover letter explaining the procedure. Reimbursement is not automatic; you must negotiate by suggesting a comparable code and fee.
Required documentation for 64999:
-
A detailed operative note describing the IPACK technique.
-
An explanation of why no specific code exists.
-
A “comparative value” code (suggest a code with similar work RVUs, such as 64450 or 64448).
-
Ultrasound images saved to the patient record (not submitted but available upon audit).
Pro Tip: When billing 64999, always attach a PDF of the procedure note. Write a brief cover letter stating: *”This unlisted code 64999 represents an ultrasound-guided IPACK block (Infiltration of Popliteal Artery and Capsular Knee). This is analogous to CPT 64450 in time, skill, and equipment.”*
Option 2: CPT 64450 – Injection, Anesthetic Agent; Other Peripheral Nerve or Branch
Some practices and billing companies use CPT 64450 for the IPACK block. They argue that the IPACK block anesthetizes “other peripheral nerves” (the genicular branches), which are not otherwise listed.
Why coders are tempted by 64450:
-
It is a recognized code that processes electronically.
-
Reimbursement is predictable (typically 0.75 to 1.0 base units plus time).
-
No need for a manual claim review.
Why 64450 is risky:
-
The IPACK block does not target a specific, named “other peripheral nerve.” It is a field block of an articular space.
-
Some auditors argue that using 64450 for IPACK is incorrect because the code is intended for blocks like the saphenous nerve, lateral femoral cutaneous nerve, or intercostals.
-
If audited, you may face a clawback of payments.
If you choose 64450, you must:
-
Document the exact nerve(s) targeted (e.g., “posterior articular branches of tibial and obturator nerves”).
-
Add modifier 59 (Distinct Procedural Service) if performed with a femoral or adductor canal block on the same knee, to avoid bundling edits.
-
Be prepared to defend your choice during a payer audit.
What About CPT 64447 or 64448? (Do NOT Use These)
A quick note on common errors: You may see forums suggesting 64448 (sciatic nerve block) for IPACK. This is incorrect and dangerous. A sciatic nerve block is a completely different procedure that causes motor weakness of the foot and ankle. Billing an IPACK as a sciatic block is fraudulent. Never use 64447 (femoral) or 64448 (sciatic) for an IPACK block.
How to Document an IPACK Block for Coding Success
Regardless of which CPT code you choose (64999 or 64450), your documentation must be flawless. Payers deny unlisted codes and audit-targeted codes due to poor documentation. Follow this checklist.
Required Elements in Your Procedure Note:
-
Indication: “IPACK block performed for postoperative analgesia for total knee arthroplasty.”
-
Technique: “Under real-time ultrasound guidance, a linear probe was placed in the popliteal fossa. The popliteal artery and the posterior knee capsule were identified. A 22-gauge, 100-mm needle was advanced using an in-plane approach. After negative aspiration, 20 mL of 0.2% ropivacaine was injected in 5 mL aliquots, visualizing hydrodissection between the artery and capsule.”
-
Ultrasound confirmation: “Spread of local anesthetic confirmed between the popliteal artery and posterior capsule.”
-
Time documentation: Start and stop time of the block procedure (separate from surgical time).
-
Laterality: Left or right knee.
-
Co-administered blocks: Note if performed with an adductor canal block (CPT 64447) or femoral nerve block.
-
Signed and dated by the provider.
Sample Documentation Snippet for an IPACK Block:
*”At the conclusion of the total knee arthroplasty, while the patient was still under general anesthesia, an ultrasound-guided IPACK block was performed on the right lower extremity. The popliteal artery and posterior knee capsule were identified in short axis. A 100mm echogenic needle was advanced from lateral to medial until the tip was positioned between the artery and capsule. After negative aspiration, 15mL of 0.25% bupivacaine with epinephrine 1:200,000 was injected. Dynamic ultrasound imaging confirmed appropriate fluid spread. No complications. Total block time: 6 minutes.”*
Billing Multiple Blocks: IPACK + Adductor Canal
In modern total knee arthroplasty, it is common to perform both an adductor canal block (CPT 64447) for anterior knee pain and an IPACK block for posterior knee pain. How do you bill this combination?
-
Adductor Canal Block: Use CPT 64447 (Injection, femoral nerve). Yes, the adductor canal block targets the saphenous nerve (a branch of the femoral), but the AMA directs coders to use 64447 for this block because no specific saphenous code exists.
-
IPACK Block: Use CPT 64999 or, if your payer accepts, 64450 with modifier 59.
Modifier use: Append modifier 59 (Distinct Procedural Service) or XU (Unusual non-overlapping service) to the second block. This tells the payer, “These two blocks are performed on different anatomic structures (anterior femoral vs. posterior capsular) and are not bundled.”
| Block | Anatomic Target | CPT Code | Modifier |
|---|---|---|---|
| Adductor Canal | Saphenous nerve (anterior knee) | 64447 | None |
| IPACK | Posterior capsular nerves | 64999 or 64450 | 59 or XU |
Payer-Specific Policies (What You Must Know)
Insurance companies do not agree on the “cpt code for ipack block.” You must research each payer’s policy. Here is a realistic overview as of early 2026.
Medicare (CMS)
Medicare does not have a national coverage determination for IPACK blocks. Local contractors (MACs) vary widely. Many MACs consider IPACK experimental or bundled into the global surgical package for TKA. Do not bill Medicare separately for an IPACK block without checking your local MAC’s policy. In many regions, you will not receive separate payment.
Commercial Payers (UnitedHealthcare, Cigna, Aetna, BCBS)
-
Most commercial payers view IPACK as a proven, medically appropriate technique for TKA.
-
They generally accept CPT 64999 (unlisted) with proper documentation.
-
Some Blue Cross plans have internal guidance to accept CPT 64450 for IPACK.
-
Always pre-authorize the block if the payer requires prior auth for peripheral nerve blocks.
Workers’ Compensation
Workers’ comp varies by state. Many states accept 64999 or 64450. However, some state fee schedules have no line item for IPACK. Contact the state workers’ comp board.
Important Note for Readers
Do not assume one code works for all payers. Before you submit a claim, call the payer’s provider line and ask: *”For an ultrasound-guided IPACK block (Infiltration of Popliteal Artery and Capsular Knee) performed for total knee arthroplasty, which CPT code do you prefer: 64999 or 64450? Do you require a modifier?” Document the representative’s name, date, and reference number.
Reimbursement Expectations (Realistic Numbers)
Because IPACK has no specific code, reimbursement varies wildly. Do not expect a fortune. Below are realistic estimates based on 2026 Medicare Physician Fee Schedule rates for a similar work RVU (0.75 to 1.0). Commercial rates are typically higher.
| Payer Type | Code Used | Estimated Reimbursement (Professional Fee) | Notes |
|---|---|---|---|
| Medicare (if paid) | 64999 (by comparison) | $40 – $70 | Rarely paid separately; often bundled |
| Commercial (64999) | 64999 | $90 – $180 | Requires paper claim and medical records |
| Commercial (64450) | 64450 | $100 – $200 | Processes automatically, but audit risk higher |
| Medicaid (varies by state) | 64999 or 64450 | $30 – $60 | Many states deny as experimental |
Facility fees (hospital outpatient): The hospital or ASC can bill separately for the IPACK block supply and equipment using HCPCS codes like G0260 (injection procedure for anesthetic agent) or unlisted surgical supply codes. This article focuses on professional fees for the physician/CRNA.
Step-by-Step Guide to Billing CPT 64999 (Unlisted)
If you decide 64999 is your best option, follow this exact workflow to reduce denials.
Step 1: Perform and document the block as described above. Save ultrasound images.
Step 2: Submit a paper CMS-1500 claim (many systems allow electronic submission with attachments, but paper is safer).
Step 3: In Box 19 (or electronic equivalent), write: *”IPACK block – see attached op note. Analogous to 64450.”*
Step 4: Attach the following:
-
Operative note describing the IPACK block.
-
Cover letter explaining the procedure, its medical necessity, and a request to pay comparable to CPT 64450 (2.15 work RVUs as of 2026).
Step 5: Follow up. If denied, appeal with literature supporting IPACK efficacy (e.g., randomized controlled trials from Regional Anesthesia & Pain Medicine).
Common Denial Reasons and How to Overcome Them
Even with perfect coding, denials happen. Here are the top three denials for IPACK block claims.
Denial 1: “Unlisted code not recognized for this service.”
-
Why it happens: The payer’s system automatically rejects 64999 for an “injection” service.
-
Fix: Call the provider line. Ask to speak to a coding specialist. Explain that no specific code exists and request a manual review.
Denial 2: “Service is bundled into the global surgical package.”
-
Why it happens: The payer considers the IPACK block part of the TKA procedure (like a local infiltration by the surgeon).
-
Fix: Argue that the IPACK block is a separate, distinct, ultrasound-guided regional anesthetic technique performed by an anesthesiologist, not the surgeon. Reference modifier 59 if appropriate.
Denial 3: “Experimental/investigational.”
-
Why it happens: Some payers have outdated policies.
-
Fix: Appeal with current medical literature (from 2020 to 2026) showing IPACK is standard of care for TKA in many institutions. Provide ASRA (American Society of Regional Anesthesia) guidelines.
Future Outlook: Will There Be a Specific CPT Code for IPACK?
The AMA CPT Editorial Panel regularly reviews new procedures. Several societies, including the American Society of Anesthesiologists (ASA) and ASRA, have submitted requests for a dedicated code for ultrasound-guided articular and pericapsular blocks (including IPACK, PENG, and others).
As of April 2026, no specific IPACK code exists. However, within the next 2-4 years, we may see a new category III code (temporary code for emerging technology) or even a category I code. Until then, use the strategies above.
Helpful Lists: Do’s and Don’ts for IPACK Coding
Do’s:
-
Do document the exact anatomic space (between popliteal artery and posterior capsule).
-
Do save ultrasound images for every block.
-
Do use an unlisted code (64999) for commercial payers when in doubt.
-
Do append modifier 59 if billing two blocks on the same knee.
-
Do check each payer’s medical policy annually.
Don’ts:
-
Don’t use 64448 (sciatic nerve block) for IPACK.
-
Don’t bill Medicare for IPACK without checking your MAC’s policy (you will likely lose).
-
Don’t forget to document start and stop times.
-
Don’t assume the surgeon’s global fee includes your block. It does not, but some payers incorrectly bundle it.
Quotation from a Coding Expert
“The single biggest mistake I see with IPACK blocks is using the sciatic nerve code (64448) because ‘it is near the popliteal fossa.’ That is a compliance disaster. Your safest path is 64999 with a strong operative note. Yes, it takes more work. But an audit defense is priceless.”
— Margaret S., CPC, CPMA, Senior Medical Coding Auditor
Additional Resources to Improve Your Knowledge
For deeper learning, visit the American Society of Regional Anesthesia and Pain Medicine (ASRA) website. They publish free white papers and coding guides for peripheral nerve blocks, including emerging techniques like IPACK.
Additional resource link:
https://www.asra.com/
(Navigate to their “Practice Management” or “Coding and Reimbursement” section for the latest updates.)
Frequently Asked Questions (FAQ)
1. What is the official CPT code for an IPACK block?
There is no official, unique CPT code for an IPACK block as of 2026. Most coders use either 64999 (unlisted procedure, nervous system) or, with caution, 64450 (injection, other peripheral nerve).
2. Can I bill an IPACK block and an adductor canal block together?
Yes. These are two distinct blocks for anterior and posterior knee pain. Bill the adductor canal block as 64447. Bill the IPACK as 64999 or 64450 with modifier 59 appended to show a distinct service.
3. Does Medicare pay for IPACK blocks?
Generally, no. Most Medicare Administrative Contractors (MACs) consider IPACK experimental or bundled into the total knee arthroplasty global package. Check your local MAC’s LCD before billing.
4. Is CPT 64448 appropriate for an IPACK block?
Absolutely not. CPT 64448 is for a sciatic nerve block, which causes motor weakness. IPACK is a capsular block that preserves motor function. Using 64448 is incorrect and may be considered fraudulent.
5. How do I bill an IPACK block if I use 64999?
You must submit a paper claim (CMS-1500) with the operative note attached. Include a cover letter explaining the procedure and requesting payment comparable to CPT 64450 based on work RVUs.
6. What documentation is required for an IPACK block to avoid denials?
You need: indication, ultrasound guidance confirmation, needle approach, local anesthetic type and volume, anatomic target (between popliteal artery and capsule), start/stop time, and saved ultrasound images.
Conclusion (Three Lines)
Finding the correct CPT code for an IPACK block requires a strategic choice between unlisted code 64999 (safest for compliance) and peripheral nerve code 64450 (easier but riskier). Successful reimbursement depends on flawless documentation, appropriate modifier use, and understanding your specific payer’s policy. Always prioritize accuracy over convenience—an audit defense is worth more than a quick payment.
Author: Clinical Coding Team
Date: APRIL 04, 2026
Disclaimer Reiterated: This information reflects best practices as of the publication date. Codes, laws, and payer policies change. Always verify with your current CPT manual and payer contracts.





