Generalized weakness is one of the most common and yet most clinically challenging symptoms presented in healthcare settings worldwide. It is a silent epidemic that cuts across all ages, genders, and backgrounds, often described by patients as a profound lack of physical strength, a feeling of being “drained,” or an overwhelming sense of exhaustion that rest does not alleviate. For the patient, it is a debilitating experience that erodes quality of life. For the clinician, it is a diagnostic puzzle with a vast and varied differential. For the medical coder, it represents a significant challenge—a symptom code that is often a placeholder for a more definitive diagnosis, requiring a nuanced understanding of clinical medicine and the rigid logic of the ICD-10-CM classification system.
The ICD-10 codes for generalized weakness, R53.1, sits at the crossroads of simplicity and complexity. On its surface, it is a single, easily located code. In practice, its appropriate application demands a meticulous review of the medical record, a deep knowledge of coding guidelines, and a collaborative relationship with healthcare providers. Misuse of this code can lead to inaccurate patient data, denied claims, and compliance issues. This comprehensive guide aims to demystify R53.1, transforming it from a default option into a precisely applied tool. We will embark on a detailed exploration of its definition, its proper use cases, the critical “excludes” notes that govern it, and the complex clinical scenarios that require a more specific code. Our goal is to equip coders, clinicians, and healthcare administrators with the knowledge to navigate this enigmatic symptom with confidence and precision.
ICD-10 Codes for Generalized Weakness
Table of Contents
ToggleChapter 1: Understanding the Symptom – What is Generalized Weakness?
Clinical Definitions and Patient Experience
Generalized weakness, in a medical context, refers to a perceived global reduction in muscle power that is not localized to a specific limb or muscle group. It is subjective, meaning it is primarily reported by the patient and may not be corroborated by objective strength testing during a physical exam. A patient might say, “I can’t climb the stairs like I used to,” “My arms feel like lead,” or “I just don’t have the energy to get through the day.”
It is crucial to distinguish this from specific neurological deficits like monoparesis (weakness of one limb) or hemiparesis (weakness of one side of the body), which point directly to a focal neurological lesion. Generalized weakness suggests a systemic issue affecting the entire body.
Differentiating Weakness, Fatigue, and Malaise
This is perhaps the most critical conceptual step for accurate coding. While these terms are often used interchangeably by patients, they have distinct clinical meanings:
-
Weakness (R53.1): Primarily refers to a lack of physical or muscular strength. The inability to perform a physical task despite the effort.
-
Fatigue (R53.83): A subjective feeling of tiredness, exhaustion, or lack of energy. It is more about a pervasive sense of weariness than a demonstrable loss of power. A person with fatigue may feel too tired to lift a grocery bag, whereas a person with true weakness may try and fail to lift it.
-
Malaise (R53.81): A general feeling of discomfort, illness, or being unwell, often at the onset of a disease. It’s a non-specific “I’m coming down with something” feeling.
In practice, these symptoms frequently coexist. A patient with influenza may experience malaise at the onset, followed by fatigue and generalized weakness. The coder’s role is to rely on the provider’s documentation. If the provider specifically documents “generalized weakness,” R53.1 is indicated. If they document “fatigue,” R53.83 should be used.
Chapter 2: The ICD-10-CM Code R53.1 – A Deep Dive
Official Code Description and Category
The code R53.1 is found in Chapter 18 of the ICD-10-CM manual, which is dedicated to Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified. Its parent code is R53 (Malaise and Fatigue).
-
Official Long Descriptor: Weakness
-
Official Short Descriptor: Weakness
This placement is significant. Chapter 18 is the repository for codes that represent problems when a more specific diagnosis has not been established. It is the “land of the unknown.”
Excludes Notes and Their Critical Importance
The “Excludes” notes are the most vital component of understanding R53.1. They are not suggestions; they are mandatory instructions that prevent double-coding and ensure diagnostic accuracy.
-
Excludes1: “asthenia NOS (R53.81)“
-
This note means that R53.1 and R53.81 are mutually exclusive. “Asthenia” is a synonym for generalized weakness. If a provider documents “asthenia” without further specification, you must code R53.81 (Other malaise), not R53.1. This is a common point of confusion.
-
-
Excludes2: “debility NOS (R53.81)” and “senile asthenia (R54)“
-
This note indicates that the conditions listed are not part of R53.1, but they can be coded with it if the patient has both. “Debility” is coded to R53.81. “Senile asthenia” is a specific code for age-related physical weakness, R54.
-
Code Also: Guiding Principles for Associated Conditions
The note “Code also any underlying condition, if known” is the golden rule for symptom coding. R53.1 should almost never stand alone if the cause of the weakness is documented. The primary code should be for the underlying etiology, and R53.1 should be assigned as a secondary code to provide additional clinical detail.
Chapter 3: The Clinical Detective Work: Linking Weakness to an Etiology
Generalized weakness is not a disease; it is a manifestation of an underlying problem. The clinician’s role is to play detective, and the coder’s role is to accurately reflect the findings of that investigation in the codes.
The Diagnostic Process and the Role of the Clinician
A thorough workup for generalized weakness may include:
-
A detailed history: Onset, duration, aggravating/relieving factors, associated symptoms (fever, weight loss, pain).
-
A review of systems: Cardiovascular, respiratory, neurological, endocrine, psychiatric.
-
A physical examination: Vital signs, cardiac and pulmonary auscultation, neurological exam, muscle strength testing.
-
Diagnostic tests: Complete blood count (CBC), comprehensive metabolic panel (CMP), thyroid-stimulating hormone (TSH), creatine kinase (CK), vitamin B12 and D levels, imaging studies.
Key Questions to Ask for Accurate Documentation
When reviewing a chart where R53.1 is considered, the coder must ask:
-
Is the weakness truly “generalized”? Or is it localized, which would point to a neurological code (e.g., G83.9 for paralysis)?
-
What is the underlying cause? Has the provider identified or suspected a specific condition?
-
Is the documentation specific? Did the provider write “weakness,” “asthenia,” “debility,” or “fatigue”? Each term has a different code.
-
Is this age-related weakness? For an elderly patient with no other identified cause, is “senile asthenia” (R54) a more accurate representation?
Chapter 4: Navigating the Coding Hierarchy – When NOT to Use R53.1
The cardinal rule of ICD-10 coding is specificity. R53.1 is a non-specific code and should be relegated to a secondary role or not used at all when a more definitive diagnosis is available.
Weakness of Known Etiology (Chapter-Specific Codes)
If the medical record establishes a causal relationship between a disease and the weakness, you must code the disease. The weakness is considered an integral part of that condition.
Examples:
-
Patient with advanced Chronic Obstructive Pulmonary Disease (COPD): Weakness is a direct consequence of hypoxia and the increased work of breathing. Code J44.9 (COPD), not R53.1.
-
Patient with Congestive Heart Failure (CHF): Weakness results from poor cardiac output and reduced perfusion to muscles. Code I50.9 (CHF), not R53.1.
-
Patient with Myasthenia Gravis (MG): This is a specific neuromuscular disorder causing weakness. Code G70.00 (Myasthenia gravis), not R53.1.
-
Patient with Chronic Kidney Disease, stage 4 (CKD): Weakness is due to uremia and anemia. Code N18.4 (CKD), not R53.1.
Using R53.1 in these scenarios would be incorrect and would misrepresent the patient’s true clinical state.
Chapter 5: Common and Complex Etiologies of Weakness – A Coding Walkthrough
Let’s explore how to code weakness in the context of common disease categories.
Weakness in Infectious Diseases (Chapter 1)
-
Scenario: Patient presents with fever, cough, and profound weakness. Diagnosed with Influenza.
-
Coding: J11.1 (Influenza with other respiratory manifestations) is the primary code. R53.1 can be added as a secondary code to emphasize the severity of the weakness, but it is not required as weakness is a typical symptom of flu.
Weakness in Neoplasms (Chapter 2)
-
Scenario: Patient with known lung cancer presents for follow-up, complaining of increasing weakness and weight loss. The provider documents “weakness due to advanced malignancy.”
-
Coding: C78.00 (Secondary malignant neoplasm of lung) or the primary lung cancer code. R53.1 and R64 (Cachexia) should be assigned as secondary codes to paint a complete picture. The “code also” instruction supports this.
Weakness in Metabolic and Endocrine Disorders (Chapter 4)
-
Scenario: Patient with uncontrolled Diabetes Mellitus type 2 complains of constant weakness. The provider attributes it to hyperglycemia.
-
Coding: E11.9 (Type 2 diabetes mellitus without complications) is the primary code. R53.1 is a secondary code.
-
Scenario: Patient diagnosed with profound hypothyroidism.
-
Coding: E03.9 (Hypothyroidism). Weakness (and fatigue) are hallmark symptoms of this condition.
Weakness in Mental and Behavioral Disorders (Chapter 5)
-
Scenario: Patient presents with anhedonia, low mood, insomnia, and reports “no energy” and “feeling weak all the time.” Diagnosed with Major Depressive Disorder, single episode.
-
Coding: F32.9 (Major depressive disorder, single episode). The “weakness” here is more accurately a manifestation of the psychomotor retardation and fatigue associated with depression. R53.1 is generally not used in this context unless the provider explicitly differentiates it from psychological fatigue.
Weakness in Neurological and Musculoskeletal Disorders (Chapters 6 & 13)
-
Scenario: Patient with Multiple Sclerosis (MS) experiences a flare-up with generalized weakness.
-
Coding: G35 (Multiple sclerosis). The weakness is a direct symptom of the demyelinating disease.
-
Scenario: Elderly patient with severe osteoarthritis and sarcopenia (age-related muscle loss) causing weakness.
-
Coding: M19.90 (Unspecified osteoarthritis) and M62.84 (Sarcopenia). R53.1 would be redundant.
ICD-10 Codes for Generalized Weakness
Chapter 6: The Power of Specificity – Sequencing and Combination Coding
The order in which codes are listed (sequencing) is as important as the codes themselves. It tells the story of the patient’s encounter.
Principal vs. Secondary Diagnosis
-
Principal Diagnosis: The condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital. For outpatient encounters, it is the reason for the visit.
-
Secondary Diagnosis: Additional conditions that coexist, or develop during the encounter, that affect patient care.
Rule: If the weakness is the reason for the encounter and no underlying cause is identified, R53.1 can be the first-listed/principal diagnosis. If an underlying cause is known, that cause becomes the principal diagnosis, and R53.1 is secondary.
Code First and Use Additional Code Notes
ICD-10-CM often provides explicit instructions.
-
Example: For Anemia, unspecified (D64.9), there is a note: “Code first any underlying cause.” If the anemia is due to chronic blood loss, you would code K92.2 (Gastrointestinal hemorrhage), then D62 (Acute posthemorrhagic anemia). The weakness would be captured by these codes.
Chapter 7: Case Studies in Clinical Practice
Let’s apply our knowledge to realistic patient scenarios.
Case Study 1: The Post-Viral Patient
-
Presentation: A 45-year-old female presents to her PCP 4 weeks after a confirmed COVID-19 infection. Her acute symptoms are gone, but she reports persistent, debilitating generalized weakness that prevents her from returning to work. The provider documents “Post-COVID-19 generalized weakness.”
-
Coding Discussion: This is a classic case for R53.1. While the cause is suspected to be post-viral, there is no specific ICD-10 code for “post-viral weakness” outside of the chronic fatigue syndrome category. The official code for the sequela of COVID-19 is U09.9 (Post COVID-19 condition, unspecified). The coding would be:
-
U09.9 (Principal diagnosis – the underlying condition)
-
R53.1 (Secondary diagnosis – the specific, lingering symptom)
-
Case Study 2: The Patient with Chronic Heart Failure
-
Presentation: A 72-year-old male with a history of CHF is admitted to the hospital because his weakness has become so severe he can no longer ambulate safely at home. The admission note states “Admitted for acute on chronic systolic heart failure exacerbation, with profound generalized weakness.”
-
Coding Discussion: The weakness is a direct symptom of the CHF exacerbation. Coding R53.1 as a principal diagnosis would be incorrect.
-
I50.21 (Acute on chronic systolic heart failure) (Principal Diagnosis)
-
R53.1 is not necessary but could be added as an optional secondary code to emphasize the presenting symptom’s severity.
-
Case Study 3: The Geriatric Patient with Multiple Comorbidities
-
Presentation: An 85-year-old female is seen in a nursing home for a gradual decline. She has osteoarthritis, hypertension, and macular degeneration. The provider’s assessment is “Senile asthenia and debility due to advanced age and multiple chronic conditions.”
-
Coding Discussion: The provider has specifically documented “senile asthenia,” which has its own code. “Debility” also points away from R53.1.
-
R54 (Age-related physical debility) (This is the most accurate code)
-
Additional codes for her chronic conditions (e.g., M19.90, I10) would also be assigned.
-
Case Study 4: Weakness as a Presenting Sign of Major Depressive Disorder
-
Presentation: A 38-year-old male presents complaining of “total body weakness” and lack of energy for 3 months. After a full medical workup reveals no abnormalities, a psychiatric consult is obtained, and he is diagnosed with Major Depressive Disorder, severe.
-
Coding Discussion: The weakness is a somatic symptom of the psychiatric disorder. The definitive diagnosis is the depression.
-
F32.2 (Major depressive disorder, single episode, severe) (Principal Diagnosis)
-
R53.1 is typically not used in this context, as the symptom is subsumed under the psychiatric diagnosis.
-
Chapter 8: Documentation Improvement – A Collaborative Effort
Accurate coding hinges on precise clinical documentation.
What Coders Need from Providers
Providers should avoid vague terms. Instead of “patient is weak and tired,” they should document:
-
“Patient reports generalized weakness, unable to rise from a chair without using arms.”
-
“Generalized muscle weakness, likely secondary to hypokalemia.”
-
“Asthenia and fatigue, out of proportion to activity.”
Querying the Provider for Clarity
If the documentation is unclear, the coder must initiate a query.
-
Example Query: “The note states the patient has ‘weakness.’ Can you please clarify if this is generalized muscular weakness, fatigue, or related to a specific neurological deficit? Additionally, is this weakness attributed to the patient’s diagnosed congestive heart failure?”
Chapter 9: The Intersection of Coding, Billing, and Compliance
The Impact of Specificity on DRGs and Reimbursement
In the inpatient setting, Diagnosis-Related Groups (DRGs) determine payment. Using a non-specific symptom code like R53.1 as the principal diagnosis often leads to a DRG with lower reimbursement and may even trigger a denial if the medical record does not support the necessity of the admission. A specific diagnosis like “Acute Decompensated Heart Failure” (I50.21) maps to a higher-weighted, more justifiable DRG.
Compliance Risks of Overusing Symptom Codes
Over-reliance on R53.1 can be a red flag for auditors. It can indicate:
-
Lack of Medical Necessity: Failing to demonstrate that a thorough investigation was performed.
-
Upcoding/Downcoding: Misrepresenting the patient’s condition.
-
Poor Documentation: A pattern of vague documentation can lead to widespread compliance issues.
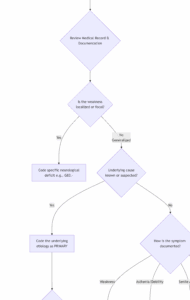
Chapter 10: Visual Guide to Coding Generalized Weakness
The following flowchart provides a step-by-step algorithm for correctly assigning a code for a patient presenting with weakness.
Differentiating Codes for Non-Specific Complaints
| Patient’s Reported Symptom | Provider’s Documentation | Most Accurate ICD-10-CM Code | Notes |
|---|---|---|---|
| “I feel weak all over.” | Generalized weakness | R53.1 | The standard code for lack of muscular strength. |
| “I have no energy.” | Fatigue | R53.83 | For tiredness/exhaustion, distinct from strength. |
| “I just feel sick and unwell.” | Malaise | R53.81 | A general feeling of being unwell. |
| “I feel weak.” (Elderly patient) | Asthenia NOS or Debility NOS | R53.81 | Excludes1 with R53.1. Must use R53.81. |
| “I’m weak from old age.” | Senile asthenia | R54 | Specific code for age-related physical debility. |
| “I’m tired and weak from my depression.” | Major Depressive Disorder | F32.9 (or other specific) | The weakness is a symptom of the mental disorder. |
Conclusion: Mastering the Nuance
Generalized weakness is a symptom that demands a coder’s highest level of scrutiny and clinical understanding. The code R53.1 is a tool of last resort when the etiology remains elusive. Always prioritize coding the definitive, underlying diagnosis first. Remember the critical “Excludes1” note for asthenia, and collaborate with providers to ensure documentation supports the most specific code possible. In doing so, you ensure coding accuracy, support quality patient data, and uphold the financial and compliance integrity of your healthcare organization.
Frequently Asked Questions (FAQs)
Q1: Can I use R53.1 as a primary diagnosis?
A: Yes, but only if the generalized weakness is the reason for the encounter and, after any workup, no underlying cause is identified. In all other cases, a more specific etiology should be sequenced first.
Q2: What is the difference between R53.1 and R54?
A: R53.1 is for general, non-specific weakness in any patient. R54 (Age-related physical debility) is specifically for weakness and frailty attributed solely to the aging process in the elderly, where no other specific disease is identified as the primary cause.
Q3: My provider constantly documents “asthenia.” What code should I use?
A: According to the ICD-10-CM Official Guidelines and the Excludes1 note under R53.1, you must code R53.81 (Other malaise) for “asthenia NOS.” You may need to educate your provider on the coding impact of using this term versus “weakness.”
Q4: A patient has cancer and weakness from chemotherapy. How do I code this?
A: You would code the specific cancer (e.g., C34.90 for lung cancer). Then, you would code R53.1 for the weakness. Finally, you would assign a code from the T80-T88 chapter to describe the adverse effect of the chemotherapy, using the appropriate external cause code.
Q5: Is there a code for Chronic Fatigue Syndrome?
A: Yes. Chronic Fatigue Syndrome is coded to G93.32 (Postviral fatigue syndrome). This is a specific diagnosis and should be used instead of R53.1 or R53.83 when documented.
Additional Resources
-
The Official ICD-10-CM Guidelines for Coding and Reporting: Published annually by the CDC and CMS. This is the ultimate authority.
-
American Health Information Management Association (AHIMA): Offers a wealth of articles, webinars, and practice briefs on coding and documentation.
-
American Academy of Professional Coders (AAPC): Provides certification, training, and forums for coding professionals.
-
CDC’s ICD-10-CM Browser Tool: An online tool to search and explore the code set.
-
Your Electronic Health Record (EHR) Vendor: Often has built-in encoders and reference materials specific to your system.
Disclaimer: This article is intended for informational and educational purposes only. It is not a substitute for professional medical coding, billing, or clinical advice. Medical coders must consult the most current, official ICD-10-CM coding guidelines, payer-specific policies, and the patient’s complete medical record to ensure accurate code assignment. The author and publisher are not responsible for any coding errors or financial repercussions resulting from the use of this information.
Date: October 1, 2025
Author: The Medical Coding Analysis Team





