Bone grafting has transformed modern medicine. It restores smiles, repairs shattered limbs, and rebuilds spines worn down by time. Yet, if you ask a surgeon, a patient, or an insurance coder a simple question—”what is a bone graft considered?”—you might receive very different answers. The truth is that a bone graft sits at a fascinating crossroads of biology and mechanics. It is a surgical procedure, but it is also a biological tool. It is a structural scaffold, yet it is a living, regenerative seed.
This guide cuts through the confusion. We will explore every facet of what a bone graft is considered, from legal billing codes to the microscopic dance of cellular biology. We will stay grounded in realistic expectations and proven science. You will walk away with a clear, thorough, and honest understanding of this medical marvel. Let’s begin the journey.
What Is a Bone Graft Considered?
Understanding the Core Definition: A Dual Identity
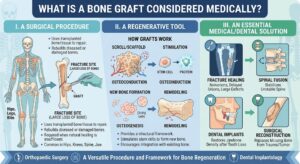
When you strip away the medical jargon, a bone graft is considered two things simultaneously. First, it is a surgical procedure, a deliberate act performed by a trained clinician. Second, it is the implant material used during that act. This material coaxes the body into doing something it sometimes forgets how to do: growing new, healthy bone.
This dual identity is the key to understanding everything else. The procedure is a mechanical and biological intervention. The material is a passive scaffold and an active biological signal. Think of it like planting a garden. The act of digging, placing the seed, and covering it is the procedure. The seed, the fertilizer, and the protective netting constitute the graft material. You need both the act and the materials to succeed.
The Surgical Procedure: A Planned Intervention
As a surgical act, what is a bone graft considered? The medical community views it as a tissue transplant. It is a scheduled, sterile operation designed to repair a skeletal defect. This defect might be a gap from a missing tooth, a non-healing fracture in a leg, or a void left after tumor removal. The surgeon accesses the site, prepares the host bone, places the graft material, and secures the area for healing.
This procedure demands precision. The surgeon must strip away scar tissue to expose a bleeding, living bone surface. This vital step creates a biological environment ready to receive the graft. Without this preparation, even the best graft material will fail. The procedure is considered reconstructive or regenerative surgery. It is not a simple injection or a superficial treatment. It rebuilds the very framework of the body.
The Biological Material: A Scaffold for Life
The material itself is a separate entity. What is a bone graft material considered? Science classifies it as a biomaterial. A biomaterial is any substance engineered to interact with biological systems for a medical purpose. Bone graft materials are unique because they are not meant to be passive forever. They are designed to be replaced by the body’s own living tissue over time.
This material provides three critical properties. It is osteoconductive, meaning it provides a scaffold for new bone to grow on. It can be osteoinductive, meaning it contains proteins that signal the body to send bone-forming cells to the site. Finally, it can be osteogenic, meaning it contains living cells ready to immediately start building bone. The source of the material—your own body, a donor, or a lab—determines which of these properties dominates. We will explore these sources in rich detail later.
The Medical Coding Perspective: What Does the Paperwork Say?
Beyond science, we live in a world of administration. To an insurance company or a hospital billing department, what is a bone graft considered? It is a specific set of codes. These codes tell a story of location, source, and complexity. Understanding this perspective helps you navigate the financial side of healing.
Medical coding uses the CPT (Current Procedural Terminology) system. Bone graft codes live in the surgical sections, generally within the 20000-29999 range for the musculoskeletal system. The codes do not just describe placing a graft. They often bundle in the graft harvest from the patient’s own body. Let’s break down this coded language.
Primary Grafting Procedure Codes
The most common codes describe the “add-on” procedure of harvesting bone. Surgeons typically use these alongside the primary surgery code. For example, the code for repairing a non-union fracture is separate from the code for obtaining the bone graft to fix it.
A core code is 20900: Bone graft, any donor area; minor or small. The surgeon might use this when taking a small amount of bone from the jaw or wrist for a dental implant. The code covers the work of making a small incision, carefully collecting the bone, and closing the site.
Next is 20902: Bone graft, any donor area; major or large. This code applies when the surgeon harvests a significant structural piece, often from the hip (iliac crest) or leg (fibula). This is a more extensive procedure with greater operative time and recovery considerations. It requires a separate incision and deeper dissection. The difference between a minor and major harvest is a critical distinction in how the surgery is considered from a billing standpoint.
The work does not stop with the harvest. The surgeon must prepare the graft. This can involve morselizing it into a paste, shaping a solid block, or mixing it with other materials. All this intraoperative work is bundled into the harvest code. It is considered an integral part of the surgical service, not a separate billable event.
Site-Specific Structural Grafts
Sometimes, the graft must replace a massive, load-bearing segment of bone. This is not a paste; it is a structural transplant. The coding system considers these procedures distinctly.
20955: Bone graft with microvascular anastomosis; fibula. This is a marathon of precision. The surgeon harvests a segment of the fibula along with its nourishing blood vessels. They then transplant it to the defect, connecting the tiny arteries and veins under a microscope. This is considered a vascularized bone graft, and it is a complex, high-stakes procedure.
20956 covers a microvascular iliac crest graft, and 20957 covers a microvascular metatarsal graft. These codes represent the pinnacle of reconstructive surgery. The graft is considered a living transplant from the moment it is disconnected and reconnected. It does not need to slowly be replaced; it survives and heals directly, just like a fracture.
A structural, non-vascularized graft has its own code: 20962: Bone graft with harvesting; other than fibular, iliac, or metatarsal. This code recognizes the technical skill of precisely shaping a dead block of donor bone to fit a complex defect mechanically. The code tells the payer that this was not a simple cavity filling but a structural reconstruction.
The Work Not Separately Coded
A crucial point of confusion is the “in conjunction with” rule. Many codes describe obtaining bone “in conjunction with” another procedure on the same surgical site. For instance, if a surgeon removes a spinal disc and performs a fusion using local bone from the vertebrae, they cannot bill separately for the graft harvest.
The harvesting is considered a component of the primary procedure. An add-on code like +20930 (Allograft, morselized, for spine surgery only) is used only for the donor bone material itself when it comes from a tissue bank, not a harvest from the patient. This distinction separates the biological material cost from the surgical work.
An important note for readers: Always verify your specific coverage. Insurance policies have unique rules on what they consider medically necessary and how they bundle payments.
The Regulatory Classification: Tissue or Drug?
A deep philosophical and legal question arises when we look at a processed bone graft material in a vial on a shelf. Is it considered a human tissue, or is it a drug? The answer changes everything about how it is regulated, sold, and used. This distinction is one of the most important yet least understood concepts for patients.
The “Minimally Manipulated” HCT/P Standard
In the United States, the FDA regulates human cells, tissues, and cellular and tissue-based products (HCT/Ps) under Section 361 of the Public Health Service Act. A bone graft from a human donor can be considered a tissue if it undergoes minimal processing. This means cleaning, shaping, freezing, or freeze-drying. It cannot be chemically altered or have its biological properties fundamentally changed.
A standard mineralized bone allograft is considered an HCT/P. The regulatory requirements focus on preventing disease transmission and contamination. The tissue bank must screen donors, test for infectious diseases, and maintain sterile processing. The FDA does not require pre-market approval for these grafts. They are considered safe when proper tissue banking standards, set by the American Association of Tissue Banks (AATB), are followed.
This path allows many traditional allografts to reach surgeons quickly. A demineralized bone matrix (DBM) putty is a borderline case. The acid demineralization process exposes bone morphogenetic proteins (BMPs), which actively induce bone formation. However, the FDA generally considers DBM minimally manipulated as long as it does not concentrate the proteins beyond their natural levels in the tissue.
The “More Than Minimally Manipulated” Drug/Device Path
Now consider a product where scientists isolate and concentrate those powerful BMPs using recombinant DNA technology. A prime example is Infuse Bone Graft (rhBMP-2). This product is not considered just a tissue scaffold. The FDA regulates it as a medical device combined with a biologic drug. It required rigorous clinical trials, FDA approval, and carries specific on-label uses and safety warnings.
The recombinant human protein is the biological drug component. The collagen sponge that holds it is the device. This combination product is considered high-risk and high-reward. It powerfully stimulates bone formation but also carries risks like severe swelling and ectopic bone formation if not used precisely. The regulatory classification here is a world apart from a simple cadaveric bone chip.
This distinction matters to you, the patient. A minimally manipulated allograft is considered safe based on a long history of clinical use and tissue banking standards. A recombinant growth factor is considered an effective but potent pharmacologic intervention that demands a thorough informed consent discussion about its unique risk profile.
Bone Grafts in Oral Surgery: The Dental Implant Gateway
In the world of dentistry, what is a bone graft considered? It is often the gateway to a functional, beautiful smile. Dental bone grafting is one of the most common surgical procedures performed today. It lays the essential foundation for the precise placement of dental implants. Without adequate bone volume, a titanium implant has no stable home.
A missing tooth leads to bone loss. The body recognizes that the jawbone in that area is no longer needed to support a root and begins to resorb it. This resorption can make a patient non-eligible for implants. The dental bone graft reverses this process. It is considered an augmentation procedure—it aims to increase the width and height of the native jawbone.
The Alveolar Ridge Preservation Graft
Imagine a tooth has just been extracted. The socket is a fresh wound. A socket preservation graft, or alveolar ridge preservation, is considered a proactive step. The surgeon places graft material directly into the extraction socket immediately after removing the tooth. This maintains the natural volume of the ridge. It prevents the collapse of the bone and gum tissue.
What is this type of graft considered from a timing perspective? It is an immediate graft. The biological goal is simple: hold space. The graft particles act as tiny placeholders, preventing the soft tissue and external pressure from collapsing the socket. Over four to six months, the body’s cells infiltrate the graft, slowly replace it with the patient’s own bone, and create a dense, healthy site ready for an implant. Skipping this step often means needing a more invasive block graft later.
The Block Bone Graft for Severe Atrophy
When the ridge has already severely melted away, a particulate graft is not enough. The surgeon needs to rebuild a three-dimensional, self-supporting structure. What is a block bone graft considered? It is the gold standard reconstructive option for severe horizontal or vertical defects.
The surgeon typically harvests a small block of bone from the patient’s jaw (like the ramus or chin) or uses a processed cadaveric block. They contour this block to fit the defect precisely and fix it to the native jaw with tiny titanium screws. This creates a rigid, stable platform. This procedure is considered more invasive than a particulate graft. It demands meticulous surgical technique, tension-free gum closure, and a longer healing period—often six months or more—before implants can be placed. The block graft is a true structural reconstruction, not just a cavity filler.
The Sinus Lift and Its Classification
The upper back teeth sit beneath the maxillary sinus, a large air-filled cavity. When these teeth are lost, the sinus floor drops down, leaving only a paper-thin layer of bone. A sinus lift, or sinus augmentation, is considered a site-development procedure. The surgeon creates a small window in the sinus wall, gently elevates the sinus membrane, and packs graft material into the new space beneath it.
This procedure is considered highly predictable. The sinus membrane itself is a powerful source of cells and blood supply for the graft. From a coding standpoint, a sinus lift has its own specific codes (e.g., D7951 for a lateral window approach). It is not coded as a simple bone graft. It is a distinct surgical act with its own complexity level. The graft material used can be a mix of allograft and xenograft (bovine bone), a combination widely considered the workhorse material for this specific anatomical challenge.
Spinal Fusion: A Structural House of Cards
Moving from the jaw to the spine, the stakes and the mechanics shift dramatically. In spinal fusion surgery, what is a bone graft considered? It is the biological cement that locks two or more vertebrae into a single, solid, pain-free column of bone. The spine is a dynamic, load-bearing structure. A failed fusion means persistent movement, potential implant failure, and ongoing pain.
Therefore, a spinal bone graft is not just a filler; it is considered a critical structural component. It must bridge a gap across a joint space, withstand the forces of daily activity, and create a continuous bony bridge that eliminates all motion. The surgeon’s technique, the choice of graft material, and the patient’s biological potential must all align perfectly.
The Posterolateral Gutter Fusion
One classic type of spinal fusion is the posterolateral gutter fusion. The surgeon lays strips of bone graft across the transverse processes of the vertebrae, outside the spinal canal, in the muscular gutters. What is the graft considered here? It is an onlay graft. It does not sit inside the disc space but bridges the bony elements on the back of the spine.
For this role, a large volume of morselized cancellous and corticocancellous bone is needed. The patient’s own iliac crest bone, harvested from the back of the hip, was long considered the gold standard. It is rich in the patient’s own living cells and growth factors. The challenge is the morbidity of the harvest site. Chronic hip pain was a significant drawback. Today, a mix of local bone from the decompression, allograft bone chips, and a biological stimulant like DBM or BMP is often considered an effective alternative, reducing the need for a separate hip incision.
The Interbody Fusion and Its Graft Demands
An interbody fusion is a different beast. Here, the surgeon removes the painful disc entirely and fills the empty space with a fusion device—a cage—packed with bone graft. What is the bone graft inside this cage considered? It is a contained, load-sharing graft. The cage bears the spinal load to prevent the graft from crushing, but the graft must then consolidate and fuse through the cage into the vertebral bodies above and below.
This environment demands a graft with excellent osteoinductive potential. The small, contained space needs a powerful biological spark. This is where rhBMP-2, the potent biologic drug discussed earlier, found its first major application. On a collagen sponge inside a metal or plastic cage, it created a robust fusion environment. However, its use in the anterior cervical spine led to dangerous swelling, leading to an FDA black box warning for that specific application. This history illustrates perfectly why a graft material’s classification (drug vs. tissue) is not a trivial regulatory matter. It is a life-and-death consideration.
The Living Graft: Free Vascularized Bone Transfer
We touched on this marvel earlier. Now, let’s give it the dedicated space it deserves. What is a free vascularized bone graft considered? It is the highest form of surgical and biological reconstruction. It is a tissue transplant and a microvascular procedure rolled into one. The surgeon moves a segment of bone, complete with its blood supply, to a distant site and reconnects it using a microscope.
The fibula is the workhorse donor. A segment of the fibula can be harvested without crippling the patient’s ability to walk. The surgeon carefully dissects out the peroneal artery and vein, which feed the fibula. The bone and its attached vessel leash are transferred to, for example, a massive defect in the lower jaw caused by cancer removal. The surgeon meticulously sutures the peroneal artery to the facial artery and the veins to nearby veins. When the tiny clamps release, the bone bleeds. It is alive.
This graft is not considered a scaffold to be replaced. It is considered a permanent, living reconstruction. It heals directly to the native jawbone like a fracture. Because it has its own blood supply, it is highly resistant to infection and can survive in a scarred, irradiated wound bed where a non-vascularized graft would surely fail. This procedure later allows for the placement of dental implants, offering a functional restoration of staggering complexity. The recovery is long, the surgery is demanding, but the result is a biological renaissance.
The Future: What Will Bone Grafts Be Considered Next?
The definition of a bone graft is not static. Tissue engineering and 3D printing are blurring the old lines. What will we consider a bone graft in the coming decade? It will be a custom-designed, bioactive, patient-specific construct built in a laboratory.
We already see the seeds. Surgeons use 3D-printed scaffolds made of bioresorbable polymers. These scaffolds match the exact shape of a patient’s defect, designed from a CT scan. They are not yet bone. They are smart, osteoconductive placeholders that slowly dissolve as the body fills the shape with natural bone. What is this considered? A synthetic bio-scaffold.
Next, consider the “living bioreactor” approach. A surgeon packs a scaffold not just with a protein but with a concentrated soup of the patient’s own stem cells, harvested from fat or bone marrow. This is a cell-based therapy. The regulatory path is complex and expensive, but the promise is a graft that recapitulates the body’s own healing ability without the morbidity of a harvest.
Finally, imagine printing a scaffold that already contains living cells and growth factors in a precise gradient, mimicking the natural architecture of bone and cartilage. This “bioprinted” construct will challenge every regulatory framework. Is it considered a tissue? A device? A manufactured organ? The answers will shape the future of medicine. The core principle, however, will remain unchanged: restoring the human body’s structural integrity and biological vitality.
Realistic Expectations and the Healing Journey
We must ground our discussion in reality. A bone graft, regardless of its source or classification, is not magic. It is the beginning of a biological process that demands time, a healthy patient, and a skilled surgeon. The procedure is considered a success only when the new bone is functional, pain-free, and stable under load.
The healing cascade is a slow, predictable symphony. First comes inflammation—a vital, necessary step that brings in the cells and signals. Next, new blood vessels invade the graft. Bone-forming cells crawl along the scaffold and begin laying down a soft, immature bone matrix called osteoid. Finally, this soft callus mineralizes and remodels in response to stress. This entire process, from graft placement to a fully mature, load-bearing fusion, takes a minimum of 6 to 12 months. For large structural grafts, it can take years.
Smoking is the nemesis of this process. Nicotine constricts blood vessels, starving the graft of oxygen and cells. A heavy smoker who undergoes a complex fusion must understand that their habit is biologically attacking the graft. Many surgeons consider smoking a relative contraindication to elective bone grafting. The failure rate skyrockets. Managing expectations means having the courage to discuss these harsh realities. A graft is a partnership between the surgeon’s skill, the material’s properties, and the patient’s responsibility to provide a healing environment.
A Practical Guide to Asking Your Surgeon the Right Questions
You are now armed with deep knowledge. Use it. When you consult with a surgeon, asking precise questions will demonstrate your engagement and help you make an informed decision. Do not hesitate to pull out a notebook. Your body, your future, is worth the dialogue.
Here is a list of questions to ask:
-
“Could you walk me through the specific CPT codes for the primary procedure and any planned bone graft harvest?” This signals you understand the coding landscape and want transparency on the surgical plan.
-
“Considering my defect, is a minimally manipulated allograft considered a sufficient solution, or does my case demand a bone morphogenetic protein drug/device combo?” This question cuts to the core of the regulatory and risk/benefit discussion.
-
“Are you planning to use my own bone? If so, from where? What is the realistic recovery pain from the donor site compared to the main surgical site?” This addresses the harvest morbidity head-on. A hip graft harvest often hurts more than the recipient site for several weeks.
-
“If we use a donor allograft, can you confirm the tissue comes from an AATB-accredited bank and what safety screening has been performed?” This shows you understand the critical importance of tissue banking standards.
-
“For my spinal fusion, what specific consideration makes you recommend a cage with cancellous chips versus a posterolateral onlay graft?” This is a technical question that forces a clear discussion about the mechanical and biological strategy.
Your surgeon will respect a well-prepared patient. This dialogue transforms the consent process from a signature on a form to a genuine shared decision-making journey.
Comparative Analysis of Bone Graft Options
To help clarify the practical differences, this table breaks down the options based on their biological properties and clinical roles.
| Graft Type | Source | Osteoconduction (Scaffold) | Osteoinduction (Growth Signals) | Osteogenesis (Living Cells) | Structural Strength | Best Clinical Use |
|---|---|---|---|---|---|---|
| Autograft (Your Own Bone) | Iliac crest, jaw, fibula | Yes | Yes | Yes | Yes (Cortical blocks) | Gold standard; non-healing fractures, large defects, spinal fusion |
| Mineralized Allograft | Cadaveric human donor | Yes | No | No | Yes | Filling bone voids, structural support in impaction grafting |
| Demineralized Bone Matrix (DBM) | Cadaveric human donor | Limited | Yes | No | No | Spinal fusion, craniofacial defects, non-unions (as a putty or strip) |
| Xenograft (Bovine/Coralline) | Animal bone or coral | Yes | No | No | Yes (Slow resorption) | Dental sinus lifts, ridge preservation (long-lasting scaffold) |
| Synthetics (Calcium Phosphates) | Lab-made | Yes | No | No | Variable | Defect filling; carrying growth factors; coating implants |
| rhBMP-2 (Infuse) | Recombinant protein | No (Needs sponge carrier) | Potently Yes | No | No | Anterior lumbar interbody fusion (ALIF); challenging non-unions |
| Vascularized Autograft | Fibula, iliac crest | Yes | Yes | Yes (Permanent) | Immediate Full Strength | Massive defect reconstruction, avascular necrosis, irradiated beds |
Frequently Asked Questions: Candid Answers from the Clinic
If a bone graft is considered a transplant, can my body reject it?
A true immunological rejection, as seen with organs, is exceptionally rare and essentially does not happen with standard bone allografts. The processing—freezing, freeze-drying—strips the donor cells and immunogenic markers. When your surgeon uses your own tissue (autograft), there is zero rejection risk. A xenograft (cow bone) is a biocompatible scaffold with no living cells to trigger rejection. What patients sometimes call “rejection” is often a simple surgical site infection or wound breakdown. The graft fails because of bacteria or poor soft tissue coverage, not immune attack. The living tissue transplant we called a vascularized free fibula does face the risk of rejection or graft-versus-host disease if the immune system is not properly managed, though this is very tightly controlled.
What is a dental bone graft considered during the waiting period for my implant?
It is considered a healing biological asset under your gums. During the 3-6 month wait, the graft is transforming. The early weeks are fragile; physical pressure or chewing can disrupt the scaffold. The particulate graft is considered a soft, mousse-like material that slowly firm up. Your surgeon considers it a success when, at the re-entry surgery, the site bleeds well and feels solid to a probe, showing it has become a vascularized, living bone-graft composite. It is not yet a dense, mature jawbone ready for an implant. That final remodeling occurs after the implant starts to function, transferring load.
If I smoke, what is my bone graft realistically considered?
It is considered a high-risk, likely-to-fail investment. A surgeon who operates on a heavy smoker knows the odds are grim. The surgical act is the same, but the biological environment is hostile. I consider such a graft a “biologically compromised scaffold.” Your money and pain may be wasted. Many ethical surgeons will refuse purely elective procedures like implants on smokers. The nicotine directly chokes the new blood vessels the graft desperately needs. Healing delays, chronic pain, and a non-union are common. The hard truth: quit completely before surgery, or accept a dramatically higher failure rate.
Deeper Context: Key Quotes from Surgical Experience
“A common mistake is thinking of a bone graft simply as a bag of cement. A bag of cement has no biological potential. It just sits there. A well-chosen bone graft, whether it’s a few chips of your own bone or a vial of DBM, is considered a partner in healing. It actively converses with the body’s cells. Our job is to create the perfect environment for that conversation to end in a solid fusion.” — An oral & maxillofacial surgeon’s practical insight.
Important Considerations Before You Consent
A final note for your decision-making checklist. A bone graft is considered an elective step in many dental cases but a non-elective, necessary procedure in major trauma or tumor reconstruction. Understand where your case falls. The recovery process is not just about the bone. The soft tissue coverage—the gums or skin over the graft—must be robust. A wound breakdown exposing the graft is the most common cause of failure. Nutrition is paramount. A body deficient in Vitamin D and calcium cannot mineralize a new scaffold. Consider the graft a beautiful house built on a weak foundation if your systemic health is poor. Heal your system, and your graft will follow.
Conclusion
A bone graft is considered a surgical transplant of biological potential, acting as a bridge between structural reconstruction and the body’s innate power of regeneration. Its identity shifts across contexts: a precise billing code, a minimally manipulated human tissue, or a potent bio-engineered drug-device combination. Understanding its dual nature as both a procedure and a living material empowers you to navigate the complexities of treatment with clear eyes and realistic hope for a restored, functional body.
Additional Resource Link:
American Association of Tissue Banks (AATB) Patient Resources: https://www.aatb.org/patients





