Carpal Tunnel Syndrome (CTS) is a ubiquitous condition, affecting millions of individuals worldwide. For patients, it manifests as a frustrating constellation of symptoms: numbness, tingling, weakness, and pain in the hand and arm, often disrupting sleep and impairing the ability to perform simple daily tasks. For clinicians, it represents a common diagnostic challenge with a well-established pathway for treatment. But for medical coders, billers, healthcare administrators, and researchers, Carpal Tunnel Syndrome is encapsulated in a precise, alphanumeric language: the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) code.
This article delves deep into the world of ICD-10 coding for Carpal Tunnel Syndrome, moving far beyond a simple listing of codes. We will explore why these codes are so much more than bureaucratic shorthand. They are the fundamental building blocks of modern healthcare data, influencing everything from individual patient reimbursement to large-scale public health initiatives. A misunderstanding or misapplication of a single character—for instance, coding G56.01 (right carpal tunnel syndrome) when the patient’s condition is bilateral (G56.03)—can trigger a chain reaction of consequences, including claim denials, inaccurate disease tracking, and flawed clinical research data.
Our journey will begin with a clear explanation of the medical condition itself, ensuring a solid foundation for understanding the coding nuances. We will then dissect the ICD-10 code family for CTS, explaining the critical importance of the 5th and 6th characters that specify laterality. Through realistic clinical scenarios, we will demonstrate how to correctly apply these codes, highlighting the indispensable link between thorough clinical documentation and accurate coding. We will also navigate the complex terrain of co-morbidities, explore the symbiotic relationship between ICD-10 diagnosis codes and CPT procedure codes, and even glance toward the future with ICD-11.
Whether you are a medical coder seeking to refine your expertise, a healthcare provider aiming to improve documentation, a student entering the health information field, or simply a curious individual wanting to understand the hidden language of healthcare, this comprehensive guide is designed to provide you with an exclusive, in-depth, and practical understanding of ICD-10 codes for Carpal Tunnel Syndrome.
ICD-10 Codes for Carpal Tunnel Syndrome
2. Understanding Carpal Tunnel Syndrome: A Primer on the Condition
Before one can master the code, one must understand the condition it represents. Carpal Tunnel Syndrome is a type of mononeuropathy, meaning it involves the compression or injury of a single peripheral nerve. In the case of CTS, the affected nerve is the median nerve.
Anatomy of the Carpal Tunnel
The carpal tunnel is a narrow, rigid passageway located on the palm side of the wrist. This tunnel is framed by the carpal bones (which form the floor and sides) and the transverse carpal ligament (which forms the roof). It is a tightly packed space through which critical structures pass:
-
The Median Nerve: This nerve provides sensation to the thumb, index finger, middle finger, and the thumb-side of the ring finger. It also controls the movement of the muscles around the base of the thumb (the thenar muscles).
-
Nine Flexor Tendons: These tendons are responsible for bending the fingers and thumb.
The Pathophysiology of CTS: Why Nerves Get Compressed
CTS occurs when the carpal tunnel becomes narrowed or when the tissues surrounding the flexor tendons swell, increasing pressure within the tunnel. This increased pressure compresses the median nerve. Like stepping on a garden hose, this compression disrupts the normal function of the nerve, leading to the characteristic symptoms:
-
Sensory Disruption: Numbness, tingling (paresthesia), and pain in the thumb, index, middle, and radial half of the ring finger.
-
Motor Dysfunction: Weakness in the hand, leading to a tendency to drop objects. In advanced cases, wasting (atrophy) of the muscles at the base of the thumb can occur.
-
Nocturnal Symptoms: Symptoms often worsen at night, as fluid redistribution and sleep postures can increase pressure in the wrist.
Common Causes and Risk Factors
While often idiopathic (meaning no single cause is identified), CTS is associated with a variety of factors that increase the risk of developing the condition:
-
Repetitive Hand Use: Jobs or activities that involve prolonged repetitive flexion of the wrist or strong gripping.
-
Anatomical Factors: A smaller carpal tunnel, which can be hereditary.
-
Medical Conditions: Diabetes, rheumatoid arthritis, hypothyroidism, and obesity can predispose individuals to nerve compression.
-
Fluid Retention: Pregnancy, menopause, and kidney failure can cause swelling that compresses the median nerve.
-
Trauma: Wrist fractures or dislocations can alter the anatomy of the tunnel.
3. The World of ICD-10-CM: Why Specificity is King
What is ICD-10-CM?
The International Classification of Diseases (ICD) is the global standard for diagnosing, managing, and classifying health conditions. Maintained by the World Health Organization (WHO), the ICD provides a common language that allows healthcare professionals to share and compare health information across the world. The Clinical Modification (CM) used in the United States is a more detailed version maintained by the Centers for Disease Control and Prevention’s National Center for Health Statistics (NCHS). It is designed for clinical and outpatient use, providing the necessary specificity for diagnosis coding in physician offices, clinics, and other non-inpatient settings.
The Shift from ICD-9: A New Era of Detail
The transition from ICD-9-CM to ICD-10-CM in the United States on October 1, 2015, was a monumental shift. ICD-9 codes were largely numeric and limited in their specificity. For example, Carpal Tunnel Syndrome had a single code: 354.0. This code did not indicate which hand was affected or whether the condition was bilateral.
ICD-10-CM introduced an alphanumeric system with codes that can be up to seven characters long. This expansion allowed for a dramatic increase in specificity. The code for CTS, G56.0-, now requires additional characters to specify laterality, a critical piece of clinical information.
4. Decoding the Codes: A Deep Dive into the Carpal Tunnel Syndrome Family (G56.0-)
The ICD-10-CM codes for Carpal Tunnel Syndrome are found in Chapter 6: Diseases of the nervous system, under the block G50-G59: Nerve, nerve root and plexus disorders. More specifically, they are categorized under G56: Mononeuropathies of upper limb.
The Parent Code: G56.0 – Carpal tunnel syndrome
This is the foundational code. However, it is never used on its own because it is an “unspecified” code. Using it would be incomplete and would likely lead to claim issues.
The Essential 5th and 6th Characters: Laterality and Specificity
The power of ICD-10 lies in these additional characters. The fifth character specifies the laterality (which side of the body is affected), and a sixth character is sometimes used for further detail.
-
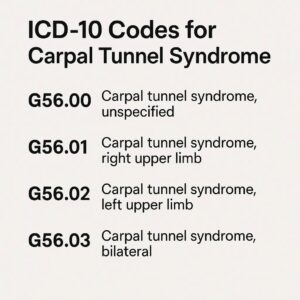
G56.01: Carpal tunnel syndrome, right upper limb – This code is used when the condition is definitively diagnosed in the right wrist.
-
G56.02: Carpal tunnel syndrome, left upper limb – This code is used when the condition is definitively diagnosed in the left wrist.
-
G56.03: Carpal tunnel syndrome, bilateral upper limbs – This code is used when the condition is definitively diagnosed in both wrists. It is crucial to note that this is a single code for the bilateral condition. You would not report G56.01 and G56.02 together for a bilateral diagnosis.
The following table provides a clear summary of the primary CTS codes:
Primary ICD-10-CM Codes for Carpal Tunnel Syndrome
5. Navigating Clinical Scenarios: Applying the Correct Codes
Theory is best understood through practice. Let’s examine how these codes are applied in real-world patient encounters.
Scenario 1: The New Patient with Unilateral Symptoms
-
Patient Presentation: A 45-year-old data entry specialist presents with a 6-month history of progressive numbness and tingling in her right thumb, index, and middle fingers. Symptoms are worse at night. Physical exam reveals a positive Tinel’s sign and Phalen’s maneuver over the right wrist. Nerve conduction studies confirm right-sided median neuropathy at the wrist.
-
Clinical Documentation: The physician’s note states: “Diagnosis: Right Carpal Tunnel Syndrome.”
-
Correct ICD-10-CM Code: G56.01
-
Rationale: The documentation clearly specifies the affected side (right). The laterality-specific code must be used.
Scenario 2: The Established Patient with Bilateral Progression
-
Patient Presentation: A patient previously diagnosed with and treated for left CTS (G56.02) returns for a follow-up. He now reports identical symptoms developing in his right hand over the past three months. Electrodiagnostic studies are repeated and confirm median nerve compression in the right wrist as well.
-
Clinical Documentation: The physician’s note states: “The patient now has bilateral carpal tunnel syndrome.”
-
Correct ICD-10-CM Code: G56.03
-
Rationale: The condition now affects both limbs. The single bilateral code G56.03 is appropriate. It replaces the previous unilateral code.
Scenario 3: Post-Surgical Follow-Up Care
-
Patient Presentation: A patient is seen for a 4-week post-operative check after undergoing an endoscopic carpal tunnel release on the left hand.
-
Clinical Documentation: The note states: “Post-operative visit following left carpal tunnel release. Patient is healing well.”
-
Correct ICD-10-CM Code: G56.02
-
Rationale: The reason for the encounter is the aftercare of the condition. The underlying diagnosis—left carpal tunnel syndrome—is still the relevant code. There are Z-code categories for aftercare (e.g., Z48.89 for other specified postprocedural aftercare), but the coding guidelines typically require listing the diagnosis code as the primary reason for the encounter when the visit is for follow-up of a chronic condition or its treatment.
Scenario 4: CTS in the Context of Pregnancy or Other Underlying Conditions
-
Patient Presentation: A 32-year-old female in her third trimester of pregnancy presents with classic bilateral CTS symptoms.
-
Clinical Documentation: The note states: “Bilateral carpal tunnel syndrome, likely related to pregnancy-induced edema.”
-
Correct ICD-10-CM Codes: G56.03 and O26.8- (Other specified pregnancy related conditions)
-
Rationale: This scenario involves two codes. First, code the condition itself (G56.03). Second, code the underlying cause or associated condition, which is pregnancy. The code from Chapter 15 (Pregnancy, Childbirth, and the Puerperium) must be sequenced first, followed by the CTS code. The coder must also add a 5th character to the O26.8 code to indicate the trimester.
6. The Documentation Link: How Physician Notes Drive Accurate Coding
Accurate coding is impossible without precise clinical documentation. The physician’s note is the source of truth for the coder.
Essential Elements in a Patient’s Chart
For coders to assign the most specific CTS code, the medical record must clearly contain:
-
A Definitive Diagnosis: The note should state “Carpal Tunnel Syndrome” or “median neuropathy at the wrist.”
-
Laterality: The single most important detail for ICD-10. The note must specify “right,” “left,” or “bilateral.”
-
Causality (if known): Any mention of an associated condition (e.g., “due to diabetes,” “associated with rheumatoid arthritis”) allows for more complete and accurate coding.
The Importance of Specifying Laterality
The shift to ICD-10 was largely driven by the need for data on laterality. From a public health perspective, knowing which side is affected can help research occupational causes. From a reimbursement perspective, payers want to ensure that procedures are billed for the correct limb. Ambiguous documentation like “patient has CTS” forces the coder to use the unspecified code G56.00, which is often seen as a red flag by payers and may lead to delayed payment or denial.
7. Common Coding Pitfalls and How to Avoid Them
Even experienced coders can make mistakes. Awareness is the first step to prevention.
-
Pitfall 1: Confusing CTS with Other Mononeuropathies. Codes from the G56.1-G56.8 range are for other nerve compressions, like ulnar neuropathy (G56.2) at the elbow (cubital tunnel syndrome). Coders must ensure the diagnosis is specifically for the median nerve at the wrist.
-
Pitfall 2: Misapplying Laterality Codes. Using two codes (G56.01 and G56.02) for a bilateral condition is incorrect. The bilateral code G56.03 exists for this exact purpose and should be used.
-
Pitfall 3: Over-reliance on Unspecified Codes. Using G56.00 should be a last resort when the documentation provides no details on laterality. The best practice is to query the physician for clarification.
8. Carpal Tunnel Syndrome and Co-morbidities: Sequencing and Combination Codes
Many cases of CTS are linked to other systemic conditions. ICD-10 has specific rules for coding these situations.
-
CTS with Diabetes Mellitus: If the CTS is directly caused by diabetic neuropathy, a combination code from the E08-E13 series with a 4th character of 4 (e.g., E11.41 – Type 2 diabetes mellitus with diabetic mononeuropathy) should be used. Do not use an additional code from G56.0- in this case, as the mononeuropathy is already included in the diabetes code.
-
CTS with Rheumatoid Arthritis: Code first the underlying condition, M05.00-M06.9 (Rheumatoid arthritis), followed by the specific CTS code (e.g., G56.03).
-
CTS with Hypothyroidism: Code first the underlying condition, E03.9 (Hypothyroidism, unspecified), followed by the specific CTS code.
9. The Role of ICD-10 in the Broader Healthcare Ecosystem
The impact of these precise codes extends far beyond a patient’s bill.
-
Billing and Reimbursement: Accurate codes are essential for clean claims. Errors lead to denials, delays, and increased administrative costs.
-
Population Health: Aggregated ICD-10 data helps public health officials track the incidence and prevalence of CTS, identify at-risk populations, and evaluate the effectiveness of treatments on a large scale.
-
Clinical Research: Researchers use coded data to identify potential participants for clinical trials, study treatment outcomes, and understand the long-term natural history of diseases like CTS.
10. Beyond ICD-10: A Look at CPT Codes for Procedures
While ICD-10 codes describe the diagnosis, Current Procedural Terminology (CPT) codes describe the procedures performed to diagnose and treat that condition.
-
Diagnostic Tests: Nerve conduction studies (e.g., CPT 95905-95907) and electromyography (e.g., CPT 95885-95886).
-
Conservative Treatment: Injection of a therapeutic agent (e.g., CPT 20526 – Injection, therapeutic; carpal tunnel).
-
Surgery: Carpal tunnel release (e.g., CPT 64721 – Neuroplasty, median nerve at carpal tunnel).
11. The Future of Medical Coding: A Glimpse at ICD-11
The WHO released ICD-11, which came into effect in January 2022. Its adoption in the U.S. will take several years. ICD-11 offers even more granularity and a modernized structure. The code for CTS in ICD-11 is 8B91.0. The coding system allows for extensive extension codes to detail severity, anatomical details, and etiological causes in a more streamlined way.
12. Conclusion: Mastering the Code for Better Patient Care
The ICD-10 code for Carpal Tunnel Syndrome is a precise tool that translates a common clinical diagnosis into actionable data. Correct application of G56.01, G56.02, or G56.03 is fundamental to ensuring accurate reimbursement, robust public health tracking, and effective clinical research. Ultimately, this precision in coding, driven by excellence in clinical documentation, supports the entire healthcare system in delivering better, more efficient, and more informed care to every patient suffering from this condition.
13. Frequently Asked Questions (FAQs)
Q1: What is the ICD-10 code for right carpal tunnel syndrome?
A: The specific code is G56.01.
Q2: Can I bill two codes (G56.01 and G56.02) if a patient has CTS in both wrists?
A: No. You should use the single code for bilateral carpal tunnel syndrome, which is G56.03.
Q3: What code do I use if the doctor’s note doesn’t specify which wrist is affected?
A: You would have to use the unspecified code G56.00. However, this is not best practice. You should seek clarification from the provider to obtain the specific laterality and use a more precise code.
Q4: How do I code for carpal tunnel syndrome caused by diabetes?
A: You would use a combination code from the E08-E13 series that includes “with diabetic mononeuropathy,” such as E11.41 for Type 2 diabetes. You would not add a separate G56.0- code.
Q5: Is there a different code for recurrent carpal tunnel syndrome after surgery?
A: There is no unique ICD-10 code for “recurrent” CTS. You would code it based on the current diagnosis and laterality (e.g., G56.01 for recurrent right CTS). The fact that it is recurrent would be indicated by the clinical documentation and may be relevant for the procedure code used for a subsequent surgery.
14. Additional Resources
-
Official ICD-10-CM Guidelines: Centers for Disease Control and Prevention (CDC) Website
-
American Academy of Professional Coders (AAPC): A leading organization for medical coders offering certifications, training, and resources.
-
American Health Information Management Association (AHIMA): A premier association for health information management professionals.
-
National Institute of Neurological Disorders and Stroke (NINDS) – Carpal Tunnel Syndrome Information Page: Provides valuable patient-oriented information on the condition itself.
Date: September 24, 2025
Disclaimer: This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. The codes and guidelines mentioned are subject to change; always refer to the most current official ICD-10-CM coding manuals and payer-specific guidelines for accurate billing and documentation.





