The skin is the human body’s largest organ, a dynamic and complex barrier that speaks volumes about our internal health. When it erupts in a rash, it is not merely a cosmetic concern; it is a symptom, a cry for help, a diagnostic puzzle. For the medical coder, a “rash” is one of the most common, yet deceptively complex, presentations they will encounter. It is a single word that can represent hundreds of distinct pathological processes, each with its own unique ICD-10-CM code. The difference between accurate and inaccurate coding in this realm is not merely a matter of reimbursement; it is a matter of patient safety, data integrity, and clinical precision.
A simple code for “unspecified dermatitis” might seem sufficient for a quick office visit, but it fails to capture the severity of a patient’s debilitating psoriasis, the allergic origin of a severe contact dermatitis, or the life-threatening nature of a drug-induced rash like Stevens-Johnson Syndrome. In the modern healthcare landscape, where data drives everything from treatment protocols to public health initiatives and value-based payments, such imprecision is no longer acceptable. This article serves as a definitive guide for medical coders, billers, clinicians, and healthcare administrators seeking to master the intricate language of ICD-10 as it applies to cutaneous eruptions. We will move beyond the superficial and delve deep into the chapters, blocks, and codes that define dermatological coding, transforming a vague “rash” into a precise, billable, and clinically meaningful diagnosis.
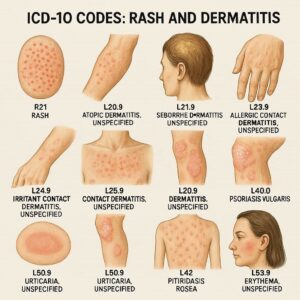
ICD-10 Code for Rashes and Dermatitis
Chapter 1: The Foundation – Understanding the L00-L99 Chapter
The ICD-10-CM Chapter 12, encompassing codes L00-L99, is dedicated exclusively to “Diseases of the skin and subcutaneous tissue.” This is the primary home for coding most rashes. Understanding its structure is the first step toward mastery.
The chapter is organized into blocks based on the etiology (cause) or morphology (structure) of the condition:
-
L00-L08: Infections of the skin and subcutaneous tissue
-
L10-L14: Bullous disorders (e.g., pemphigus, pemphigoid)
-
L20-L30: Dermatitis and eczema
-
L40-L45: Papulosquamous disorders
-
L49-L54: Urticaria and erythema
-
L55-L59: Radiation-related disorders of the skin and subcutaneous tissue
-
L60-L75: Disorders of skin appendages (e.g., nails, hair, sweat glands)
-
L80-L99: Other disorders of the skin and subcutaneous tissue
A crucial initial step is confirming that the rash is indeed a primary skin condition. Many systemic diseases manifest with skin findings. For example, the classic “butterfly rash” of lupus erythematosus is coded not to Chapter 12, but to M32.- (Systemic lupus erythematosus) in Chapter 13. Similarly, a rash caused by a viral infection like measles is coded to B05.- (Measles) in Chapter 1. The golden rule is: code the underlying cause, not just the symptom.
Chapter 2: The Workhorse Code – Unspecified Dermatitis (L30.9) and Its Pitfalls
L30.9 (Dermatitis, unspecified) is one of the most frequently used codes in dermatology. It is also one of the most misused. This code should be a last resort, employed only when the clinical documentation provides no further detail beyond the generic term “rash” or “dermatitis.”
While it may facilitate billing in the short term, over-reliance on L30.9 has significant drawbacks:
-
Clinical Ambiguity: It provides no useful information for tracking disease prevalence or outcomes.
-
Reimbursement Risks: Payers are increasingly scrutinizing unspecified codes and may deny claims or downcode them, arguing that a more specific diagnosis should have been established.
-
Quality Metrics: In value-based care models, the use of unspecified codes can negatively impact a practice’s quality scores and performance payments.
The coder’s role is to work collaboratively with clinicians. If a provider documents “rash,” the coder should query the provider for more specificity. Is it eczematous? Is it contact-related? Is it localized or generalized? This proactive approach elevates the entire revenue cycle and clinical data management process.
Chapter 3: The Eczema Spectrum (L20-L30)
The terms “eczema” and “dermatitis” are often used interchangeably and refer to a group of conditions characterized by inflammation, itching, redness, and sometimes blistering and weeping.
3.1 Atopic Dermatitis (L20.-)
Atopic dermatitis is a chronic, relapsing, intensely pruritic inflammatory skin condition often associated with a personal or family history of atopy (asthma, allergic rhinitis).
-
L20.0: Besnier’s prurigo (a severe, chronic form)
-
L20.81: Atopic neurodermatitis
-
L20.82: Flexural eczema
-
L20.83: Infantile (acute) (chronic) eczema
-
L20.84: Intrinsic (allergic) eczema
-
L20.89: Other atopic dermatitis
-
L20.9: Atopic dermatitis, unspecified
Specificity is key. Documenting the specific type, such as “flexural eczema,” allows for the use of a more precise code.
3.2 Seborrheic Dermatitis (L21.-)
This common condition affects areas rich in sebaceous glands, such as the scalp (dandruff), face, and chest. It presents with greasy, yellowish scales on erythematous patches.
-
L21.0: Seborrhea capitis (cradle cap in infants, dandruff in adults)
-
L21.1: Seborrheic infantile dermatitis
-
L21.8: Other seborrheic dermatitis
-
L21.9: Seborrheic dermatitis, unspecified
3.3 Contact Dermatitis (L23-L25)
This block is a masterclass in ICD-10 specificity. It requires the coder to identify the causative agent.
-
L23 (Allergic contact dermatitis): This is a delayed-type hypersensitivity reaction.
-
L23.0: Due to metals (e.g., nickel, chromium)
-
L23.2: Due to cosmetics
-
L23.5: Due to chemicals in rubber, plastics, etc.
-
L23.6: Due to food in contact with the skin
-
L23.7: Due to plants (e.g., poison ivy, oak, sumac)
-
-
L24 (Irritant contact dermatitis): This is a non-allergic inflammatory reaction caused by direct chemical or physical damage to the skin.
-
L24.0: Due to detergents
-
L24.2: Due to oils and greases
-
L24.5: Due to other chemicals
-
-
L25 (Unspecified contact dermatitis): Used when the provider documents “contact dermatitis” but does not specify allergic or irritant, and does not identify the cause.
Coding Tip: Always use an additional code from categories Z77.- (Contact with and (suspected) exposure to hazardous substances) to identify the specific substance if known, for example, Z77.098 (Contact with and (suspected) exposure to other hazardous metals) for a nickel allergy.
Chapter 4: The World of Papulosquamous Disorders (L40-L45)
This group of disorders is characterized by scaly (squamous) papules and plaques.
4.1 Psoriasis (L40.-)
Psoriasis is a chronic immune-mediated disease with several distinct phenotypes.
-
L40.0: Psoriasis vulgaris (plaque psoriasis) – The most common form.
-
L40.1: Generalized pustular psoriasis (von Zumbusch) – A severe, life-threatening form.
-
L40.2: Acrodermatitis continua – Pustular psoriasis of the fingertips and toes.
-
L40.3: Pustulosis palmaris et plantaris – Pustules on palms and soles.
-
L40.4: Guttate psoriasis – Characterized by small, drop-like lesions, often triggered by streptococcal infection.
-
L40.5: Arthropathic psoriasis (L40.50-L40.59) – Psoriasis associated with joint inflammation. This requires an additional code from M07.0-M07.3 to specify the type of psoriatic arthropathy.
-
L40.8: Other psoriasis (e.g., inverse psoriasis)
-
L40.9: Psoriasis, unspecified
4.2 Lichen Planus (L43.-) and Pityriasis Rosea (L42)
-
Lichen Planus: An inflammatory condition causing purplish, itchy, flat-topped papules.
-
L43.0: Hypertrophic lichen planus
-
L43.1: Bullous lichen planus
-
L43.2: Lichenoid drug reaction – Code first the drug (T36-T50)
-
L43.3: Subacute (active) lichen planus
-
L43.8: Other lichen planus (e.g., erosive)
-
L43.9: Lichen planus, unspecified
-
-
Pityriasis Rosea (L42): A self-limiting condition characterized by a “herald patch” followed by a widespread, Christmas-tree-like distribution of scaly patches.
Chapter 5: Urticaria, Erythema, and Vascular Reactions (L49-L54)
These conditions involve vascular changes in the skin, leading to redness, wheals, and sometimes systemic symptoms.
5.1 Urticaria (L50.-)
Urticaria, or hives, is characterized by transient, itchy wheals.
-
L50.0: Allergic urticaria
-
L50.1: Idiopathic urticaria
-
L50.2: Urticaria due to cold and heat
-
L50.5: Cholinergic urticaria (triggered by heat, exercise, stress)
-
L50.6: Contact urticaria
-
L50.8: Other urticaria (e.g., vibratory)
-
L50.9: Urticaria, unspecified
5.2 Erythema Multiforme (L51.-) and Stevens-Johnson Syndrome/TEN (L51.1-L51.3)
This is a critical area where coding accuracy is paramount due to the potential severity of the conditions.
-
L51.0: Non-bullous erythema multiforme – The milder form, often associated with herpes simplex virus.
-
L51.1: Stevens-Johnson syndrome (SJS) – A severe, life-threatening skin blistering condition affecting <10% of body surface area (BSA).
-
L51.2: Toxic epidermal necrolysis (TEN) – The most severe form, affecting >30% BSA.
-
L51.3: Stevens-Johnson syndrome-toxic epidermal necrolysis (SJS-TEN) overlap – Affecting 10-30% BSA.
-
L51.8: Other erythema multiforme
-
L51.9: Erythema multiforme, unspecified
Crucial Coding Instruction: Codes from L51.- require an additional code to identify the cause. If drug-induced, the drug must be coded first (T36-T50 with fifth or sixth character 5). For example:
-
T36.0x5A (Adverse effect of penicillins, initial encounter)
-
L51.1 (Stevens-Johnson syndrome)
Chapter 6: Infections and Infestations Presenting as Rash (A00-B99)
Many rashes are not primary skin diseases but symptoms of an underlying infection. The coder must be vigilant.
-
Bacterial: Cellulitis (L03.-), Impetigo (L01.-), Erysipelas (A46)
-
Viral: Herpes Zoster (Shingles – B02.-), Varicella (Chickenpox – B01.-), Herpes Simplex (B00.-), Measles (B05.-)
-
Fungal: Candidiasis of skin (B37.2), Tinea corporis (ringworm – B35.4), Tinea pedis (athlete’s foot – B35.3)
-
Infestations: Scabies (B86), Pediculosis (lice – B85.-)
The morphology of the rash (vesicles in herpes, annular plaques in tinea, burrows in scabies) provides the diagnostic clue that points the coder to the correct chapter.
Chapter 7: Drug Eruptions – The Critical Link to the T Code (L27.- & T36-T50)
Drug-induced rashes are common and can range from mild to fatal. ICD-10 provides specific codes for these reactions.
-
L27.- (Dermatitis due to substances taken internally): This category is for more generalized rashes like morbilliform (measles-like) drug eruptions.
-
L27.0: Generalized skin eruption due to drugs and medicaments
-
L27.1: Localized skin eruption due to drugs and medicaments
-
-
Other Specific Drug Eruptions: As discussed, urticaria (L50.-), erythema multiforme (L51.-), and lichenoid reactions (L43.2) can all be drug-induced.
The Coding Sequence is Non-Negotiable:
-
Code first the nature of the adverse effect. Use a code from T36-T50 with the 5th or 6th character ‘5’ (e.g., T45.1X5A for adverse effect of anticoagulants).
-
Then, code the specific manifestation. Use the appropriate code from L27.-, L50.-, L51.-, etc.
Example: A patient develops a generalized morbilliform rash after starting Amoxicillin.
-
T36.0x5A: Adverse effect of penicillins, initial encounter
-
L27.0: Generalized skin eruption due to drugs and medicaments
Chapter 8: The Art of Documentation – From Clinician to Coder
Accurate coding is impossible without precise documentation. Clinicians must provide a “paint-by-numbers” picture for the coder.
8.1 Location, Location, Location
Many codes have extensions for anatomical site.
-
Psoriasis: L40.0- (requires a 5th digit for site: L40.52 for scalp psoriasis)
-
Pressure Ulcer: L89.- (requires a 5th digit for stage and a 6th digit for site)
8.2 Laterality and Specificity
ICD-10 demands laterality.
-
L60.2: Onycholysis (unspecified finger)
-
L60.21: Onycholysis of right finger
-
L60.22: Onycholysis of left finger
8.3 Severity and Chronicity
While not always a direct part of the code, documenting “acute,” “chronic,” “severe,” or “mild” supports medical necessity for the level of service provided.
Chapter 9: Common Pitfalls and How to Avoid Them
-
Pitfall: Defaulting to L30.9.
-
Solution: Query the provider. Ask: “Can the rash be described further (e.g., eczematous, papulosquamous)?”
-
-
Pitfall: Coding the rash instead of the underlying systemic disease.
-
Solution: Ask: “Is this rash a symptom of a larger condition (e.g., lupus, viral infection)?”
-
-
Pitfall: Incorrectly sequencing drug eruptions.
-
Solution: Remember the rule: T code first, manifestation code second.
-
-
Pitfall: Ignoring laterality and site specificity.
-
Solution: Use the ICD-10 index and tabular list to find the most specific code available. Never assume a code is “good enough.”
-
Chapter 10: The Future of Dermatological Coding – A Look Ahead
The evolution of ICD-10 is ongoing. We can expect further granularity, potentially incorporating more details about disease severity, treatment resistance, and genetic markers. The integration of artificial intelligence (AI) in clinical documentation may also assist in automatically suggesting the most specific codes based on clinical notes and even clinical images. The coder’s role will evolve from data entry to that of a data quality manager, ensuring the AI’s suggestions are clinically accurate and compliant.
Chapter 11: Practical Scenarios and Coding Tables
To solidify these concepts, let’s examine a table of common clinical scenarios and their corresponding codes.
ICD-10 Coding Scenarios for Common Rashes
| Clinical Scenario | Provider Documentation | Primary ICD-10 Code(s) | Rationale & Additional Codes |
|---|---|---|---|
| Scenario 1 | “Patient presents with chronic, itchy, scaly plaques in elbow flexures and popliteal fossae. Diagnosis: Atopic Dermatitis.” | L20.83 (Infantile eczema) or L20.84 (Intrinsic eczema) or L20.89 (Other atopic) | The specific type of atopic dermatitis should be coded. L20.9 is a fallback if no detail is given. |
| Scenario 2 | “Rash on wrist under new nickel-plated watch. Pruritic, erythematous, vesicular. Diagnosis: Allergic Contact Dermatitis to nickel.” | L23.0 (Allergic contact dermatitis due to metals) | Consider adding Z77.098 (Contact with and exposure to other hazardous metals). |
| Scenario 3 | “Patient with known plaque psoriasis presents with new joint pain and swelling in hands. Diagnosis: Psoriatic Arthritis.” | L40.54 (Psoriatic arthritis mutilans) OR other L40.5- code | AND M07.61 (Arthritis mutilans, shoulder) or other specific joint code from M07.6-. Two codes are required. |
| Scenario 4 | “Generalized hives 30 minutes after taking Amoxicillin for sinusitis. Diagnosis: Acute Urticaria due to Penicillin.” | T36.0x5A (Adverse effect of penicillins) L50.0 (Allergic urticaria) |
The T code for the drug is sequenced first, followed by the manifestation (urticaria). |
| Scenario 5 | “Widespread blistering rash and skin sloughing affecting 15% BSA, onset one week after starting allopurinol. Diagnosis: SJS-TEN Overlap.” | T50.4x5A (Adverse effect of drugs affecting uric acid metabolism) L51.3 (SJS-TEN overlap) |
A life-threatening emergency. Correct sequencing is critical for data tracking and severity adjustment. |
| Scenario 6 | “Child presents with diffuse, fine, sandpaper-like rash, strawberry tongue, fever. Rapid strep test positive. Diagnosis: Scarlet Fever.” | A38.9 (Scarlet fever, uncomplicated) | This is an infectious disease, not a primary skin condition. Code to Chapter 1. |
*(Image: A flowchart titled “Decision Tree for Coding a Rash.” It starts with “Patient Presents with Rash,” then asks: “Is it a symptom of a systemic/infectious disease? (e.g., fever, specific pattern)” -> If YES, code to the underlying condition (A00-B99, M00-M99, etc.). If NO, proceed to “Identify Morphology/Etiology” (Eczema, Papulosquamous, Urticaria, etc.) -> Then, “Assign code from L00-L99” -> Finally, “Check for required additional codes (T codes for drugs, M codes for arthritis, Z codes for exposure).”)*
Conclusion
Mastering ICD-10 coding for rashes requires a meticulous, detail-oriented approach that bridges clinical understanding and administrative precision. It demands moving beyond the generic term “rash” to capture the specific etiology, morphology, and location of the cutaneous eruption. By leveraging detailed documentation, understanding the structure of the L00-L99 chapter, and correctly applying sequencing rules—especially for adverse effects—coders can ensure accuracy, optimize reimbursement, and, most importantly, contribute to high-quality patient data that fuels clinical research and effective public health strategies.
Frequently Asked Questions (FAQs)
Q1: What is the single most important thing a provider can do to help with accurate rash coding?
A1: Provide specific and detailed documentation. Avoid using the word “rash” alone. Describe the morphology (e.g., plaques, papules, vesicles), the distribution (e.g., generalized, flexural, sun-exposed), the suspected etiology (e.g., “allergic contact dermatitis due to poison ivy”), and the chronicity.
Q2: When do I use L27.0 vs. L50.0 for a drug reaction?
A2: Use L27.0 for generalized, non-specific drug eruptions (like a morbilliform or “maculopapular” rash). Use L50.0 when the drug reaction specifically presents as urticaria (hives or wheals). The clinical description of the lesion is the deciding factor.
Q3: How do I code a rash that is documented as “eczema” but the type is not specified?
A3: If no further detail is available (e.g., not specified as atopic, contact, etc.), you would default to L30.9 (Dermatitis, unspecified). However, a query to the provider for clarification is always the best practice.
Q4: A patient has psoriasis and develops a separate rash from poison ivy. How do I code both?
A4: You code both conditions. The primary diagnosis would be the reason for the encounter. If the patient is being seen for the acute, severe poison ivy rash, you would code L23.7 (Allergic contact dermatitis due to plants) as the first-listed diagnosis, and the patient’s pre-existing L40.0 (Psoriasis vulgaris) as a secondary, chronic diagnosis.
Q5: Are there any official guidelines I should be following for ICD-10-CM?
A5: Yes. The ICD-10-CM Official Guidelines for Coding and Reporting, published by the CDC and CMS, are the definitive authority. They are updated annually and provide specific instructions on conventions, sequencing, and chapter-specific rules that must be followed.
Additional Resources
-
CDC ICD-10-CM Official Guidelines: https://www.cdc.gov/nchs/icd/icd-10-cm.htm (The primary source for all coding rules).
-
American Academy of Dermatology (AAD): https://www.aad.org (Provides clinical resources and practice management tools that can aid in documentation).
-
American Health Information Management Association (AHIMA): https://www.ahima.org (Offers credentials, education, and resources for coding professionals).
-
American Academy of Professional Coders (AAPC): https://www.aapc.com (Provides certification, training, and networking for medical coders in all specialties, including dermatology).
Date: October 24, 2025
Author: Dr. Evelyn Reed, MD, MPH, CPC
Disclaimer: The information contained in this article is intended for educational and informational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or coding practice. The author and publisher are not responsible for any errors or omissions or for any consequences resulting from the use of this information.





