If you have ever looked at a lab requisition form or a medical bill, you have likely seen a jumble of numbers and letters next to the reason for a blood draw. These are ICD-10 codes. They are the universal language of diagnosis in the healthcare world.
For patients, they can seem like random data. But for medical billers, coders, lab managers, and even healthcare providers, understanding how to correctly apply ICD-10 codes for lab tests is crucial. It determines whether a lab gets paid, whether a claim is denied, and whether the patient’s medical record accurately reflects their health journey.
This guide is designed to be your friendly roadmap through this complex landscape. We will avoid dry, academic language. Instead, we will walk through real-world scenarios, explain the rules in plain English, and give you the tools to ensure that every lab test ordered has a code that tells the right story.
We are not here to give you a simple list (those are available in code books). We are here to help you understand why a specific code is used, how to link it to a test, and how to avoid common pitfalls that lead to rejected claims.
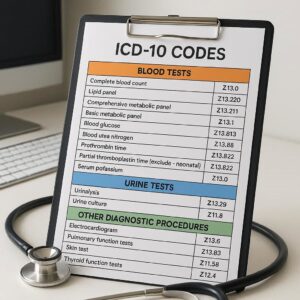
ICD-10 Codes for Lab Tests
The Golden Rule of Lab Coding: Sign vs. Diagnosis
Before we dive into specific codes, we need to address the single most important concept in laboratory coding. It is also the most common source of confusion and claim denials.
The rule is simple: For routine lab testing, you almost never code the final diagnosis before the test is run.
Think about it. A doctor doesn’t know you have diabetes when they order an A1c test. They suspect it, or they are monitoring it. When ordering the test, the patient presents with a problem. In the world of ICD-10, we code what we know at the time of the order.
-
Signs: Objective evidence of a disease observed by the doctor (e.g., a rash, a fever, a mass).
-
Symptoms: Subjective evidence experienced by the patient (e.g., fatigue, pain, nausea).
-
Diagnosis: A confirmed conclusion after evaluating the signs, symptoms, and test results.
For lab test orders, the ICD-10 code should reflect the sign, symptom, or reason for the test, not the suspected diagnosis.
Important Note: Payers (insurance companies) need to see “medical necessity.” They need to know why the doctor is spending money on a test. “Because I wanted to check for diabetes” isn’t a valid reason. “Because the patient is excessively thirsty and urinating frequently” is a valid reason. The code tells that story.
The “Unacceptable” Diagnoses: Why Screening Codes Matter
There is a specific category of ICD-10 codes that often causes a stir: the Z00-Z99 range, known as “Factors Influencing Health Status and Contact with Health Services.”
When it comes to lab tests, the most relevant of these are the screening codes (Z11-Z13) .
A screening code is used when a test is performed on a patient who has zero signs or symptoms of a disease. It is a proactive measure.
-
Scenario A: A 50-year-old man comes in because he has blood in his stool. The doctor orders a colonoscopy. This is a diagnostic test based on a sign. You would use a code for the symptom (blood in stool).
-
Scenario B: A 50-year-old man comes in for a routine physical. He feels great, has no digestive issues, but is due for his screening colonoscopy based on his age. The doctor orders the test. This is a screening. You would use a screening code (e.g., Z12.11 for screening for malignant neoplasm of colon).
Why You Can’t Always Use a Screening Code
While screening codes are valid, payers often have strict rules about them. They may only pay for specific screenings at specific ages or intervals (like a Pap smear every 3 years). If a patient comes in for a “screening” but had the same test six months ago, the claim may be denied.
Furthermore, you cannot use a screening code if a symptom is present. If the patient has a symptom, the symptom code takes priority because it establishes medical necessity for a diagnostic workup.
Common Lab Tests and Their Corresponding ICD-10 Codes (By Scenario)
Now, let’s get practical. We will look at common lab tests and walk through the thought process of choosing the right code. Remember, these are examples, and the specific patient chart must always support the code used.
1. Basic Metabolic Panel (BMP) / Comprehensive Metabolic Panel (CMP)
These are workhorse tests that look at kidney function, glucose levels, and electrolyte balance.
| Patient Scenario (The Story) | What you code (ICD-10) | Code Description |
|---|---|---|
| Patient complains of persistent fatigue and unintentional weight loss. | R53.83 | Other fatigue |
| R63.4 | Abnormal weight loss | |
| Patient has known hypertension and is taking a diuretic; doctor wants to check kidney function and potassium levels. | I10 | Essential (primary) hypertension |
| Z79.82 | Long-term (current) use of diuretics | |
| Patient feels perfectly fine but is due for an annual wellness visit. | Z00.00 | Encounter for general adult medical examination without abnormal findings |
| Patient presents with severe vomiting and diarrhea for 3 days (risk of dehydration/electrolyte imbalance). | R11.2 | Nausea with vomiting, unspecified |
| R19.7 | Diarrhea, unspecified |
2. Lipid Panel (Cholesterol Test)
This measures cholesterol and triglycerides, crucial for cardiovascular health.
| Patient Scenario (The Story) | What you code (ICD-10) | Code Description |
|---|---|---|
| Patient is obese and has a family history of early heart attacks. Doctor orders a lipid panel to assess risk. | E66.9 | Obesity, unspecified |
| Z82.49 | Family history of ischemic heart disease and other diseases of the circulatory system | |
| Patient is a 35-year-old male with no risk factors, here for a routine employment physical. | Z02.1 | Encounter for pre-employment examination |
| Patient with known high cholesterol is on a statin; doctor wants to see if the medication is working. | E78.5 | Hyperlipidemia, unspecified |
| Z79.899 | Other long-term (current) drug therapy (for the statin) |
3. Hemoglobin A1c (Diabetes Monitoring/Diagnosis)
This test provides a 3-month average of blood sugar levels.
| Patient Scenario (The Story) | What you code (ICD-10) | Code Description |
|---|---|---|
| Patient complains of excessive thirst (polydipsia) and frequent urination (polyuria). | R63.1 | Polydipsia |
| R35.81 | Nocturia (frequent urination at night) | |
| Patient with Type 2 diabetes comes in for a routine 3-month check-up. | E11.9 | Type 2 diabetes mellitus without complications |
| Patient is pre-diabetic and needs to monitor their progress after starting a diet and exercise plan. | R73.03 | Prediabetes |
| Patient is pregnant and being screened for gestational diabetes. | Z34.90 | Encounter for supervision of normal pregnancy, unspecified, unspecified trimester |
Important Note: Notice how we used R73.03 (Prediabetes) for the patient monitoring their condition. Prediabetes is a condition that can be coded, but it is distinct from a confirmed diagnosis of diabetes (E11.-).
4. Complete Blood Count (CBC)
This test evaluates red cells, white cells, and platelets. It is used for a huge variety of reasons.
| Patient Scenario (The Story) | What you code (ICD-10) | Code Description |
|---|---|---|
| Patient reports feeling dizzy and looks pale. Doctor suspects anemia. | R42 | Dizziness and giddiness |
| R23.1 | Pallor | |
| Patient has a persistent fever and a cough. Doctor wants to check white blood cell count to look for infection. | R50.9 | Fever, unspecified |
| R05 | Cough | |
| Patient is on a medication known to potentially suppress bone marrow function (like chemotherapy or certain immunosuppressants). | Z79.899 | Other long-term (current) drug therapy |
| Patient complains of easy bruising and bleeding gums. | R23.3 | Spontaneous ecchymosis (bruising) |
| R68.81 | Bleeding from gums, unspecified |
5. Urinalysis (UA)
A simple but powerful test for kidney and metabolic issues.
| Patient Scenario (The Story) | What you code (ICD-10) | Code Description |
|---|---|---|
| Patient complains of burning during urination and urinary frequency. | R30.0 | Dysuria (painful urination) |
| R35.0 | Frequency of micturition | |
| Patient’s urine looks dark or cloudy. | R39.12 | Cloudy urine |
| Annual physical for a patient with a history of kidney stones. | Z87.442 | Personal history of (corrected) urinary calculi |
Navigating the Gray Areas: “R” Codes and Medical Necessity
You may have noticed the heavy use of codes starting with the letter “R” in the examples above. These are the Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified codes.
These “R” codes are the bread and butter of laboratory coding. They are honest. They say, “We don’t have the answer yet, but here is the problem we are trying to solve.”
However, some coders and providers worry that using an “R” code looks less serious or less likely to be paid than a definitive “E” (Endocrine) or “I” (Circulatory) code. This is a misunderstanding.
-
Use an “R” code when appropriate: If a patient has fatigue, code fatigue (R53.83). If a lab finding came back abnormal from a previous test, and you are doing a new test to follow up, you can code the abnormal finding (e.g., R79.9 for abnormal blood chemistry finding).
-
Do not “upcode”: Never use a diagnosis code that has not been officially confirmed by a physician just to make a claim look more payable. This is fraud. If the patient does not have a documented diagnosis of diabetes, you cannot use an E11 code.
When Can You Use a Confirmed Diagnosis Code with a Lab Test?
There are two primary scenarios where you can (and should) use a confirmed diagnosis code when ordering a lab test:
-
Monitoring a Known Condition: As we saw in the lipid panel example. The patient has hyperlipidemia (E78.5). The lab test is not to find the condition, but to manage it. The diagnosis code is valid because the condition is already part of the patient’s medical history.
-
Pre-Procedure or Pre-Operative Testing: A patient with confirmed coronary artery disease (I25.10) who is scheduled for non-cardiac surgery might need a baseline CBC and BMP. The diagnosis code for the procedure (Z01.810 for pre-procedural cardiovascular examination) might be used, or the underlying chronic condition that necessitates the testing.
The Critical Role of “Z” Codes: More Than Just Checkups
We touched on screening codes earlier, but the “Z” code chapter offers much more. These codes add layers of context to a lab test order that can be vital for justifying medical necessity.
Common “Z” Codes Used in Lab Testing
-
Z00-Z13 (Encounter for medical examinations): As discussed, for annual physicals, school physicals, and employment physicals.
-
Z68 (Body mass index [BMI]): A high or low BMI can support the medical necessity for tests like lipid panels or nutritional deficiency tests. For example, a patient with a BMI of 31 (Z68.31) is at higher risk for metabolic issues, justifying a proactive screening.
-
Z77-Z99 (Persons with potential health hazards related to family and personal history and certain conditions influencing health status):
-
Z79.- (Long-term drug therapy): This is a hugely important category.
-
Z79.82 (Long-term use of aspirin): Can justify certain cardiac-related labs.
-
Z79.84 (Long-term use of oral hypoglycemic drugs): Supports the need for an A1c to monitor diabetes control.
-
Z79.899 (Other long-term drug therapy): For medications like statins, diuretics, or thyroid replacements that require regular blood monitoring.
-
-
Z82-Z84 (Family history): A family history of conditions like diabetes (Z83.3), high cholesterol (Z83.42), or certain cancers can justify screening tests even in asymptomatic patients.
-
Example: Putting It All Together
Let’s build a complete and defensible coding scenario for a lab requisition.
The Patient: A 55-year-old woman.
The Chart/Doctor’s Notes:
-
Patient is here for a follow-up. She has Type 2 diabetes (E11.9) and takes Metformin (Z79.84).
-
She is also on a statin for high cholesterol (E78.5).
-
She mentions she has been feeling more tired than usual lately (R53.83).
-
Due to her age and family history of breast cancer (Z80.3), a screening mammogram is also ordered (though not a lab test, it shows the principle).
The Lab Order & Codes:
-
Hemoglobin A1c: To monitor diabetes control.
-
Primary Code: E11.9 (Type 2 diabetes without complications)
-
Secondary Code: Z79.84 (Long-term use of oral hypoglycemic drugs)
-
-
Comprehensive Metabolic Panel (CMP): To monitor kidney function (common in diabetics) and check electrolytes.
-
Primary Code: E11.9 (Type 2 diabetes without complications)
-
Secondary Code: R53.83 (Other fatigue – this adds the reason for checking for things like electrolyte imbalance that could cause fatigue).
-
-
Lipid Panel: To monitor cholesterol control on statin therapy.
-
Primary Code: E78.5 (Hyperlipidemia, unspecified)
-
Secondary Code: Z79.899 (Other long-term drug therapy)
-
In this example, every test is linked to a specific, justifiable reason that is documented in the patient’s chart.
Common Pitfalls and How to Avoid Them
Even experienced billers can stumble. Here are some of the most frequent errors seen in lab coding, and how to steer clear of them.
Pitfall 1: The “Rule Out” Trap
This is the biggest one. A doctor writes in their note: “Rule out myocardial infarction.” or “R/O Diabetes.” The coder then uses codes for myocardial infarction (I21.9) or diabetes (E11.9) on the lab order.
The Fix: You cannot code for a condition that is being “ruled out.” Code the signs and symptoms that prompted the doctor to suspect the condition. For “R/O MI,” you would code chest pain (R07.9) or shortness of breath (R06.02). For “R/O Diabetes,” you would code polydipsia (R63.1) or fatigue (R53.83).
Pitfall 2: Coding from the Result, Not the Order
A lab receives a requisition for a Vitamin D level with the code M79.1 (Myalgia – muscle pain). The result comes back showing a severe deficiency (E55.9). The biller thinks, “We should change the code to E55.9 because that’s the truth!”
The Fix: The ICD-10 code on the claim must reflect the patient’s condition at the time the test was ordered. The doctor ordered the test because of muscle pain. M79.1 is the correct code for that encounter. The diagnosis of Vitamin D deficiency (E55.9) will be used for future visits to manage the condition, but not for the test that discovered it.
Pitfall 3: Using Unspecified Codes When a Specific One Exists
Using a code like R53.81 (Other malaise) when the notes specifically say “fatigue” (R53.83). Or using I10 (hypertension) when the notes specify “hypertensive heart disease with heart failure” (I11.0).
The Fix: Always code to the highest level of specificity that the medical record supports. This paints a more accurate picture and is required for proper reimbursement under HIPAA.
Pitfall 4: Forgetting the “Z” Codes for Context
Ordering a CBC and BMP for a patient on a medication that can affect blood counts or kidney function, but only coding the underlying condition (e.g., rheumatoid arthritis).
The Fix: Always add the Z79 code for long-term drug use. It explicitly tells the payer, “This test is necessary because of the side effects of this medication,” which is a powerful justification for medical necessity.
A Closer Look: ICD-10 Codes for Specialized Lab Testing
While the principles remain the same, some areas of laboratory medicine have their own unique coding considerations.
Microbiology and Infectious Disease
When a doctor orders a culture to identify a pathogen, the coding is usually straightforward.
-
Scenario: Patient has a suspected urinary tract infection (UTI).
-
Symptoms: Burning with urination (dysuria) and foul-smelling urine.
-
Correct Codes: R30.0 (Dysuria) and R39.15 (Foul-smelling urine).
-
What not to use: N39.0 (Urinary tract infection, site not specified). You cannot confirm it’s a UTI until the culture results come back positive.
Therapeutic Drug Monitoring
This is for patients on medications with a narrow therapeutic range, where too little is ineffective and too much is toxic (e.g., Warfarin, Digoxin, Lithium, certain antiseizure medications).
-
Scenario: Patient with a mechanical heart valve is on Warfarin (Coumadin) to prevent blood clots. The doctor orders a PT/INR test.
-
Correct Code: Z79.01 (Long-term (current) use of anticoagulants). This is a perfect example of a “Z” code establishing medical necessity. You might also code the underlying condition, like Z95.2 (Presence of prosthetic heart valve).
Genetic Testing
This is a rapidly growing field. The coding depends heavily on the reason for the test.
-
Diagnostic: A patient with symptoms of a genetic disorder (e.g., unexplained developmental delays) undergoes testing. Code the signs/symptoms (e.g., F88 for other disorders of psychological development).
-
Pre-symptomatic: A patient with a strong family history of Huntington’s disease wants to know their status. Code Z84.89 (Family history of other specified conditions) or Z13.79 (Encounter for screening for genetic and chromosomal anomalies).
-
Pharmacogenomic: A patient is about to start a medication and the doctor wants to test how their liver enzymes will metabolize it. Code Z13.79 (Encounter for screening for genetic and chromosomal anomalies) or Z01.89 (Encounter for other specified special examinations), depending on the payer’s preference.
The Lab Requisition Form: A Checklist for Accuracy
Before a lab test is even drawn, the accuracy of the coding can be determined by the information on the requisition form. Whether paper or electronic, ensure it has these components:
-
Patient Demographics: Correct name, date of birth, and ID number. Mismatched info is a top reason for claim rejection.
-
Ordering Provider Information: Full name and NPI (National Provider Identifier). The claim will be denied if the payer can’t identify who ordered the test.
-
Diagnosis Codes: At least one ICD-10 code, and ideally up to four, that directly support the medical necessity of each test ordered.
-
Tests Ordered: Specific, unambiguous test names (e.g., “Hemoglobin A1c,” not just “diabetes panel”).
-
Signature and Date: The provider’s signature and the date the test was ordered. Verbal orders must be authenticated within a certain timeframe.
Pro Tip: If you are a patient, you have the right to ask your doctor’s office what diagnosis code they are using for a lab test. If you see a code for a condition you don’t have, speak up! It could be a simple clerical error that might affect your insurance or future medical records.
How Technology is Changing Lab Coding
The days of paper requisitions and manual code lookups are fading. Technology is playing a huge role in improving accuracy.
-
Computer-Assisted Coding (CAC): These systems use natural language processing (NLP) to “read” the physician’s notes and suggest appropriate ICD-10 codes. For example, if the doctor writes “patient complains of headache and blurred vision,” the system might suggest R51 (Headache) and H54.8 (Blurred vision). The coder still reviews and approves, but it saves time and reduces human error.
-
Electronic Health Records (EHR) with Decision Support: Modern EHRs can flag potential issues before the order is even sent.
-
If a doctor tries to order a hemoglobin A1c test for a patient with no diabetes history and no symptoms, the system might pop up a warning: “This patient does not have a diagnosis supporting this test. Please select a reason from the list below (e.g., screening, polyuria).”
-
This real-time feedback is invaluable for preventing denials.
-
-
Clearinghouses and Claim Scrubbing: Before a claim is sent to the insurance company, it often goes through a “clearinghouse.” These are electronic services that run the claim through a series of automated checks. They can catch things like a diagnosis code that is invalid for the patient’s gender or age, or a mismatch between the test and the diagnosis code (e.g., a pregnancy test ordered for a 75-year-old man).
Conclusion
Navigating the world of ICD-10 codes for lab tests is less about memorizing thousands of codes and more about understanding a simple narrative. You are telling the story of why a test is needed using the information available at that specific moment. By focusing on signs, symptoms, and the context of the patient’s health history, you can ensure that every code you use is accurate, ethical, and defensible. Mastering this process protects your practice from denied claims and, most importantly, ensures that the patient’s medical record is a true reflection of their healthcare journey.
Frequently Asked Questions (FAQ)
1. What is the difference between a diagnosis code and a procedure code for labs?
A diagnosis code (ICD-10) explains the reason for the test (e.g., R53.83 for fatigue). A procedure code (CPT/HCPCS) describes the actual test performed (e.g., 80061 for a lipid panel). Both are required on a claim.
2. Can I use the same ICD-10 code for multiple lab tests on the same day?
Yes, absolutely. One diagnosis code can support multiple tests. For example, a code for hypertension (I10) can support both a BMP (to check kidney function) and a lipid panel (to check cardiovascular risk).
3. What happens if I use the wrong ICD-10 code on a lab claim?
Several things can happen. The claim may be denied, and the lab won’t get paid. It could be paid but later flagged for audit, requiring you to pay the money back. In cases of deliberate fraud, it can lead to legal penalties.
4. My doctor wrote “annual labs” on the order. What code should be used?
“Annual labs” is not a specific reason. You should look for the reason for the annual visit. If it’s a routine physical with no complaints, use a Z00.00 code. If the patient has a chronic condition like diabetes, use the diabetes code as the primary reason for monitoring.
5. Where can I look up ICD-10 codes?
You can use online tools from the CDC (Centers for Disease Control and Prevention) which maintains the official ICD-10 code set. Many medical billing software platforms also have built-in code lookup tools.
6. What does “medical necessity” mean in simple terms?
It means the test is reasonable and necessary for the patient’s condition. In other words, there is a logical connection between the patient’s symptoms or known condition (the ICD-10 code) and the test the doctor ordered (the CPT code).
Additional Resource
For the most up-to-date and authoritative information on ICD-10 coding, you should always refer to the official source. The Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) are the governing bodies for these codes in the United States.
-
Link: CMS ICD-10 Home Page
Disclaimer: The information provided in this article is for general informational purposes only and does not constitute legal, billing, or coding advice. Medical coding regulations, payer policies, and guidelines are subject to change. Always consult with a qualified coding professional or refer to the official ICD-10 coding manuals and payer-specific guidelines for definitive information.





