If you are navigating the world of foot and ankle surgery coding, you have likely encountered the term “McBride bunionectomy.” It is a classic procedure, but when it comes to assigning the correct CPT code, things can get a little tricky. You are not alone if you find yourself flipping through your coding manual or second-guessing whether to use 28292 or a different code altogether.
This guide is designed to clear up that confusion. We will walk through what a McBride bunionectomy actually is, which CPT code applies to it, how to distinguish it from similar procedures, and the documentation you need to support your claim. Whether you are a coder, a biller, a medical assistant, or a patient trying to understand your surgery estimate, this article will provide the clarity you need.
CPT Code for McBride Bunionectomy
What Is a McBride Bunionectomy?
Before we talk about codes, we need to talk about the surgery itself. Medical coding is built on precision. If you do not understand the anatomy and the surgical steps, you cannot accurately assign the code.
A McBride bunionectomy is a specific type of surgical correction for a bunion, medically known as hallux valgus. A bunion is a bony bump that forms at the base of the big toe, causing the big toe to angle toward the second toe. Over time, this can lead to pain, inflammation, and difficulty walking.
The History Behind the Name
The procedure is named after Dr. Edward D. McBride, an orthopedic surgeon who popularized this technique in the early 20th century. Unlike more aggressive bunion surgeries that involve cutting the bone (osteotomy), the traditional McBride procedure is a soft tissue procedure.
How the McBride Procedure Works
The primary goal of the McBride bunionectomy is to realign the structures around the big toe joint without necessarily cutting the bone. The key steps typically include:
-
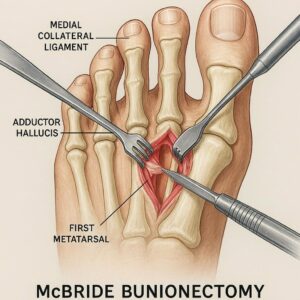
Lateral Release: The surgeon releases the tight structures on the outer side of the big toe joint. This involves cutting the adductor hallucis tendon and the lateral joint capsule. These are the structures that pull the big toe outward toward the second toe.
-
Medial Capsular Plication: The surgeon tightens the loose capsule on the inner side of the big toe.
-
Exostectomy (Bump Removal): The surgeon removes the bony prominence (the “bump”) on the side of the first metatarsal head. This is often done with a specialized saw or chisel.
-
Possible Bunionette Correction: Sometimes, the procedure is combined with a correction for a tailor’s bunion (bunionette) on the fifth toe, though this is less common.
The key takeaway here is that the classic McBride bunionectomy relies primarily on soft tissue balancing and removal of the bony bump. It does not involve cutting and repositioning the first metatarsal bone.
The Primary CPT Code: 28292
Now, let us get to the heart of the matter. The most accurate CPT code for a traditional McBride bunionectomy is CPT 28292.
The official descriptor for CPT 28292 is:
Correction, hallux valgus (bunionectomy), with sesamoidectomy
However, there is a nuance that confuses many coders. Historically, the descriptor for 28292 included specific language about the McBride type procedure. While the current descriptor focuses on “sesamoidectomy,” the standard of care and coding guidelines confirm that 28292 is the appropriate code for the McBride bunionectomy when the procedure includes the lateral release, medial capsular repair, and exostectomy.
What Is a Sesamoidectomy?
A common point of confusion is the mention of “sesamoidectomy” in the code descriptor. The sesamoids are two small bones located beneath the first metatarsophalangeal (MTP) joint. In a traditional McBride procedure, the surgeon often removes the tibial sesamoid (the one on the inner side) or performs a partial resection to allow the big toe to shift back into alignment.
If the surgeon performs the McBride technique without removing a sesamoid, you might question whether 28292 still applies. In most cases, payers expect 28292 for this procedure package. If the surgeon documents a McBride bunionectomy without mention of sesamoid work, it is best to verify the operative report to ensure the code aligns.
When to Use 28292
You should report 28292 when the operative report clearly indicates:
-
A lateral release (adductor hallucis tendon release).
-
A medial capsular reefing or plication.
-
An exostectomy (removal of the bony prominence).
-
Documentation of a McBride-type procedure or a “soft tissue bunionectomy.”
-
Typically, a sesamoidectomy or sesamoid work.
The “Other” Bunionectomy Code: 28296 vs. 28292
One of the most frequent coding errors is confusing 28292 with CPT 28296. These two codes are not interchangeable. Selecting the wrong one can lead to claim denials, audits, and lost revenue.
Let us break down the difference in a simple comparative table.
| Feature | CPT 28292 | CPT 28296 |
|---|---|---|
| Procedure Type | Soft tissue correction with sesamoidectomy | Osteotomy (bone cutting) |
| Bone Work | Exostectomy (bump removal) only | Cutting and realigning the first metatarsal |
| Key Components | Lateral release, medial capsular repair, removal of bony prominence, sesamoid work | Proximal or distal metatarsal osteotomy with internal fixation (screws, pins, or plates) |
| Common Name | McBride bunionectomy, soft tissue bunionectomy | Chevron, Scarf, or other osteotomy bunionectomy |
| Fixation | Usually none, or possibly a pin for temporary stabilization if needed | Typically requires internal fixation (screws, wires) |
Why This Distinction Matters
If a surgeon performs a chevron osteotomy (cutting the bone into a V-shape and shifting it) and you code 28292, you are under-coding and potentially leaving money on the table. However, more importantly, you are misrepresenting the service.
Conversely, if a surgeon performs a soft tissue McBride and you code 28296, you are up-coding, which is a compliance risk. Payers look for the presence of internal fixation (screws) when they see 28296. If the operative report does not describe an osteotomy with fixation, the claim will likely be denied or flagged for review.
Documentation Requirements for 28292
To successfully bill for a McBride bunionectomy using 28292, the operative report must tell a complete story. Insurance companies do not accept just the procedure name. They require detailed documentation that supports the medical necessity and the specific components of the code.
Essential Elements in the Operative Report
Here is what a coder should look for in the surgeon’s notes:
-
Medical Necessity: A clear diagnosis of hallux valgus. The most common ICD-10 code is M20.10 (Hallux valgus, unspecified foot) or a more specific code depending on laterality and severity. The report should describe the degree of angulation and the patient’s symptoms (pain, difficulty with footwear).
-
Specific Laterality: The report must clearly state which foot was operated on (left or right). If bilateral procedures are performed, you will need to append modifier -50 (Bilateral procedure) to the CPT code, or report the code twice with modifiers -LT (Left) and -RT (Right), depending on payer preference.
-
Soft Tissue Work Description: The report must explicitly mention the release of the adductor hallucis tendon and the lateral joint capsule. It should also describe the medial capsular reefing or plication.
-
Bone Work Description: The report must detail the removal of the exostosis (the bunion bump). Even if the surgeon is performing a classic McBride, the bony prominence is always addressed.
-
Sesamoidectomy (If applicable): If a sesamoid is removed, the report should specify whether it was the tibial or fibular sesamoid and whether it was a partial or complete resection.
-
Absence of First Metatarsal Osteotomy: Critically, the report should not describe an osteotomy of the first metatarsal. If the surgeon cuts the first metatarsal to reposition it, 28292 is no longer the correct code.
A Note on Modifiers
If the surgeon performs a McBride bunionectomy on the right foot and a different procedure (like a hammertoe correction) on the same foot, you will need to append modifier -51 (Multiple procedures) to the secondary code. If the surgery is performed on both feet during the same operative session, modifier -50 is typically used.
Reimbursement and Payer Considerations
Navigating reimbursement for 28292 requires understanding that not all payers view this procedure the same way. While 28292 is a valid and established code, some insurance carriers have specific policies regarding bunion surgery.
Global Period
CPT 28292 carries a 90-day global period. This means that all routine post-operative care related to the surgery is included in the reimbursement for the first 90 days after the procedure. You cannot bill separately for routine follow-up visits, dressing changes, or staple/suture removal during this period unless there is a distinct, unrelated complication.
Medicare and Commercial Payers
Medicare and most commercial payers cover bunionectomy when it is medically necessary. However, “cosmetic” bunion surgery is not covered. The documentation must prove that the patient has significant pain, deformity, and functional impairment.
Some payers have begun to scrutinize the use of 28292 versus 28296. They may use automated auditing software to check if an X-ray was performed, if the diagnosis severity is appropriate (e.g., mild, moderate, or severe hallux valgus), and if the documentation matches the code.
Common Denial Reasons
If your claim for 28292 is denied, here are the most common reasons:
-
Missing X-ray documentation: Payers want to see radiographic evidence of the bunion angle.
-
Cosmetic exclusion: The diagnosis code does not indicate pain or functional impairment.
-
Code mismatch: The operative report describes an osteotomy, but 28292 was billed.
-
Missing modifiers: Bilateral procedures were performed but modifiers were omitted.
-
Incorrect place of service: Ensuring the place of service code (e.g., 24 for ambulatory surgical center, 11 for office) matches the facility where the surgery occurred.
McBride Bunionectomy vs. Other Bunion Procedures
To solidify your understanding, let us look at how the McBride (28292) stacks up against other common bunion procedures. This will help you quickly differentiate when you are reviewing operative notes.
1. McBride Bunionectomy (28292)
-
Best for: Mild to moderate hallux valgus, especially in younger, active patients where preserving the joint is a priority.
-
Key Feature: No cutting of the first metatarsal. Soft tissue balancing is the star of the show.
-
Recovery: Often involves earlier mobilization compared to osteotomy procedures, though weight-bearing restrictions may still apply based on surgeon preference.
2. Chevron/Scarf Osteotomy (28296)
-
Best for: Moderate to severe hallux valgus.
-
Key Feature: The surgeon cuts the first metatarsal (distally or proximally) and shifts it laterally to correct the angle. This almost always involves internal fixation like screws or wires.
-
Recovery: Typically requires a period of non-weight-bearing or protected weight-bearing to allow the bone to heal.
3. Lapidus Procedure (28297)
-
Best for: Severe hallux valgus with instability at the tarsometatarsal (TMT) joint.
-
Key Feature: Fusion of the first metatarsal to the medial cuneiform bone.
-
Recovery: Longer recovery due to fusion site healing; strict non-weight-bearing is common.
4. Keller Bunionectomy (28290 – a deleted code)
Note: CPT 28290 (Keller procedure) was a distinct code for a resection arthroplasty, but it has been deleted in recent years. Procedures that were previously coded as 28290 are now generally captured by 28292 or 28296, depending on the technique.
Here is a quick-reference list to help you remember the primary bunionectomy codes:
-
28292: McBride, soft tissue, with sesamoidectomy.
-
28296: Osteotomy (chevron, scarf) with internal fixation.
-
28297: Lapidus, arthrodesis (fusion) of first metatarsal-cuneiform joint.
-
28298: Osteotomy with proximal phalanx (Akin osteotomy).
-
28299: Triple procedure (osteotomy + fusion + soft tissue).
Real-World Scenarios: Applying the Code
Let us look at a few scenarios to see how a coder would arrive at the decision to use 28292.
Scenario 1: The Classic McBride
Operative Report Summary: A 45-year-old female with painful hallux valgus of the right foot. A curvilinear incision was made over the medial aspect of the first MTP joint. The exostosis was resected using a sagittal saw. The adductor hallucis tendon was released from the lateral aspect. The lateral capsule was incised. The tibial sesamoid was partially excised. The medial capsule was then reefed and imbricated to realign the hallux.
Coding Decision: CPT 28292. The report includes exostectomy, lateral release, medial reefing, and sesamoidectomy. No osteotomy of the first metatarsal is described.
Scenario 2: Soft Tissue Work with a Question Mark
Operative Report Summary: Patient undergoes bunionectomy. Surgeon documents: “The bunion bump was removed. A lateral release was performed. The medial capsule was tightened. No osteotomy was performed.”
Coding Decision: This is a bit ambiguous. While the procedure sounds like a McBride, the surgeon did not document a sesamoidectomy. In many coding circles, this still falls under 28292 because the code descriptor includes “with sesamoidectomy,” but the procedure package for a soft tissue bunionectomy implies that sesamoid work is inherent. However, to be safe, the coder should query the surgeon to confirm if sesamoid work was performed. If the surgeon confirms no sesamoid work was done, some payers may still accept 28292, while others might require a different code. Always query when documentation is unclear.
Scenario 3: The Mixed Procedure
Operative Report Summary: Surgeon performs a McBride-type soft tissue release and exostectomy but also performs a proximal phalangeal osteotomy (Akin osteotomy) on the big toe to correct a distal deformity.
Coding Decision: CPT 28298. This code is specifically for “correction, hallux valgus, with osteotomy, proximal phalanx.” It is more comprehensive. You would not report 28292 in addition to 28298 because the work is bundled.
Common Pitfalls and How to Avoid Them
Even experienced coders can stumble over bunionectomy coding. Here are the top pitfalls to watch out for when dealing with 28292.
Pitfall 1: Assuming “Bunionectomy” Equals 28292
Not all bunionectomies are McBride procedures. The term “bunionectomy” is often used generically by surgeons in their documentation. You cannot rely on the procedure name alone. You must read the operative report to determine if bone was cut or if only soft tissue was addressed.
Pitfall 2: Overlooking Modifier -59
If a surgeon performs a McBride bunionectomy and a separate, distinct procedure on the same foot (such as a hammertoe correction, CPT 28285), you must use modifier -59 (Distinct procedural service) or -XS (Separate structure) to indicate that these are separate and distinct procedures. Without this modifier, the payer may bundle the hammertoe correction into the bunionectomy payment.
Pitfall 3: Billing for Unlisted Procedures
Sometimes, coders get nervous and default to an unlisted procedure code (e.g., 28899) for a “modified” McBride. This should be a last resort. If the procedure meets the general description of 28292, use it. Unlisted codes almost always result in manual review, delayed payment, and a high likelihood of denial if the medical records are not submitted preemptively.
Pitfall 4: Forgetting the Global Period
Do not bill for routine post-op care separately. If the patient returns two weeks after surgery for suture removal, that is included in the global period. If the patient returns four weeks post-op for a new injury unrelated to the surgery, you can bill that with modifier -24 (Unrelated evaluation and management service during a post-operative period).
Tips for Accurate Coding and Reimbursement
To wrap up the technical side, here are some actionable tips to ensure your claims for 28292 are clean and paid promptly.
-
Standardize Your Operative Report Templates: Work with your surgeons to create templates that require them to check boxes or fill in blanks for key elements like “Exostectomy performed,” “Lateral release performed,” “Sesamoidectomy performed (yes/no),” and “First metatarsal osteotomy (yes/no).” This eliminates ambiguity.
-
Use ICD-10 Specificity: Do not just use M20.10. If the patient has bilateral hallux valgus, use M20.11 (right) and M20.12 (left). If the condition is severe or involves other digits, use the appropriate codes to support medical necessity.
-
Append Modifiers Immediately: Create a workflow where modifiers are checked before the claim goes out. A missing -LT/-RT or -50 is one of the most common reasons for a claim to pend or deny.
-
Stay Updated: CPT codes change. While 28292 has been stable for years, the deletion of 28290 (Keller) was a significant shift. Keep an eye on the American Medical Association (AMA) and American Academy of Professional Coders (AAPC) updates annually.
-
Educate on Payer Policies: Some regional Medicare Administrative Contractors (MACs) or local commercial payers may have specific Local Coverage Determinations (LCDs) regarding hallux valgus correction. These LCDs often specify what imaging is required and what severity of deformity warrants surgery. Always check your local payer policies.
What Patients Should Know About CPT Codes
If you are a patient reading this, you might be wondering why this matters to you. When your surgeon’s office schedules your bunion surgery, they will provide you with an estimate that includes CPT codes. Understanding these codes can help you:
-
Verify Insurance Coverage: You can call your insurance company and ask them if they cover CPT 28292 for the diagnosis of hallux valgus. This gives you clarity on your out-of-pocket costs.
-
Compare Estimates: If you receive estimates from different surgical facilities, ensure they are using the same CPT code. Comparing 28292 to 28296 is like comparing apples to oranges—the complexity and cost structures are different.
-
Understand Your Bill: When your Explanation of Benefits (EOB) arrives, you can look for the code to ensure the service you received matches what was billed.
Additional Resources
For those looking to dive deeper into coding for foot and ankle surgery, having the right references at your fingertips is crucial. Here are a few trusted resources to keep in your library:
-
American Academy of Professional Coders (AAPC): Their forums and coding books are invaluable for real-world advice and official coding guidelines.
-
American Medical Association (AMA) CPT® Professional Edition: This is the official source for CPT code descriptors and guidelines. It is essential to have the most current edition.
-
American Orthopaedic Foot & Ankle Society (AOFAS): They often publish coding articles and updates specifically for orthopedic foot and ankle surgeons and coders. Their resources help bridge the gap between surgical technique and billing compliance.
-
Local Coverage Determinations (LCDs): Search for your local Medicare Administrative Contractor (MAC) to review their LCDs for bunion surgery. This will tell you exactly what documentation they require for reimbursement.
Frequently Asked Questions (FAQ)
1. Is 28292 the only code for a McBride bunionectomy?
Yes, in the vast majority of cases, 28292 is the specific CPT code used to report a traditional McBride bunionectomy. It includes the lateral release, exostectomy, and soft tissue repair. If the surgeon adds a bone-cutting procedure (osteotomy) to the McBride, then a different code, such as 28296 or 28298, would be more appropriate.
2. What is the difference between CPT 28292 and 28296?
The primary difference lies in the bone work. 28292 is a soft tissue procedure that does not involve cutting the first metatarsal bone. 28296 involves an osteotomy (cutting and realigning) of the first metatarsal, typically requiring internal fixation like screws or pins. Choosing the wrong code is one of the most common reasons for claim denials.
3. Does CPT 28292 include a sesamoidectomy?
Yes, the official descriptor for 28292 includes “with sesamoidectomy.” In practice, the soft tissue balancing performed during a McBride procedure often necessitates partial or complete removal of the tibial sesamoid. If the surgeon performs all the other steps of a McBride but does not touch the sesamoid, the coder should review the documentation to confirm if 28292 is still the best choice based on payer guidelines.
4. What is the global period for bunion surgery code 28292?
CPT 28292 has a 90-day global period. This means that the surgical reimbursement covers all routine post-operative care for 90 days following the procedure. You cannot bill separately for follow-up visits, suture removal, or routine check-ups during this time unless there is a distinct, unrelated complication.
5. Can I bill for a McBride bunionectomy on both feet at the same time?
Yes, if the surgeon performs bilateral McBride bunionectomies during the same operative session, you should report the code with modifier -50 (Bilateral procedure). Alternatively, some payers prefer to see the code reported on two lines with modifiers -LT (Left) and -RT (Right). Check your specific payer’s guidelines for their preference.
6. What diagnosis code should I use with 28292?
The primary diagnosis code is usually M20.10 (Hallux valgus, unspecified foot) or a more specific code such as M20.11 (Hallux valgus, right foot) or M20.12 (Hallux valgus, left foot). The documentation must clearly support medical necessity, including pain, deformity, and functional limitation. A diagnosis of “bunion” alone without associated symptoms may be denied as cosmetic.
7. Is the McBride bunionectomy still performed today?
Yes, but it is performed less frequently than osteotomy procedures like the chevron. The McBride remains an excellent option for patients with mild to moderate hallux valgus, particularly younger patients with good joint mobility and minimal arthritic changes. It is often preferred when the goal is to avoid cutting the bone and to allow for a potentially quicker recovery of soft tissue.
Conclusion
Navigating the CPT code for a McBride bunionectomy does not have to be a source of stress. To summarize the key takeaways: the correct code is CPT 28292. This code represents a soft tissue correction that includes lateral release, medial capsular repair, exostectomy, and typically a sesamoidectomy. The most critical distinction to remember is that 28292 does not involve cutting the first metatarsal; if bone realignment is performed, you are likely looking at a different code such as 28296. By focusing on precise documentation, proper modifier usage, and a clear understanding of the surgical procedure, you can ensure accurate coding, compliant billing, and appropriate reimbursement.
Additional Resource Link:
For the most current official CPT coding guidelines and to purchase the latest CPT Professional Edition, visit the American Medical Association (AMA) website: www.ama-assn.org





