Navigating the world of medical billing for hormone replacement therapy requires absolute precision. One minor mistake can lead to an immediate claim denial or significant underpayment. For healthcare providers administering testosterone replacement therapy (TRT), a frequent point of confusion centers around identifying the correct hcpcs code for testosterone cypionate 200mg.
If you look at an old coding manual, you might see a dedicated code for a 200 mg dose. However, standard modern billing relies on a per-milligram unit calculation strategy. This guide breaks down the active coding rules, step-by-step unit multipliers, essential modifiers, and common pitfalls to ensure your claims are clean, compliant, and reimbursed fully.
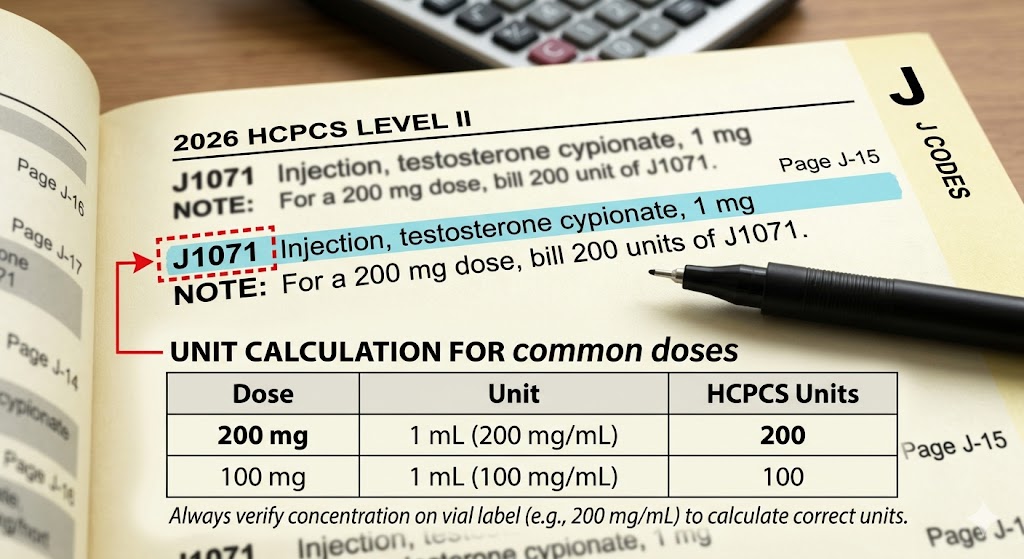
The Primary Code: HCPCS Code J1071
The standard, active code for reporting testosterone cypionate injections is HCPCS code J1071.
The official long description established by CMS reads:
“Injection, testosterone cypionate, 1 mg”
The crucial detail here is the 1 mg dosage unit. Unlike historical codes that covered an entire pre-packaged vial size as a single billing unit, J1071 measures your billing output incrementally by the exact milligram administered.
Why You Cannot Use Old Codes Like J1080
Years ago, medical billers relied on code J1080 (Injection, testosterone cypionate, 1 cc, 200 mg). This code was officially deleted by CMS on December 31, 2014. Attempting to submit J1080 on a modern electronic CMS-1500 claim form will trigger an immediate clearinghouse rejection or a hard denial for using an inactive code.
Brand Name vs. Generic Billing
Whether you are administering generic testosterone cypionate or the well-known brand-name version Depo-Testosterone, HCPCS code J1071 remains your primary choice. The code applies to any standard, multi-dose or single-dose vial formulation of the drug given via intramuscular injection.
Calculating Billing Units for a 200 mg Dose
Because the descriptor for J1071 specifies 1 mg = 1 billing unit, you must calculate your units based on the total mass of the drug delivered to the patient, not the fluid volume in milliliters (mL).
Testosterone cypionate is most commonly supplied in a concentration of 200 mg/mL. If you administer a standard 1 mL injection of this concentration, you have delivered 200 mg of the medication.
The Unit Multiplier Formula
To find the correct quantity to place in Box 24G (Days or Units) of the CMS-1500 claim form, use the following simple calculation:
$$\text{Total Milligrams Administered} \div \text{HCPCS Code Unit Allowance} = \text{Billable Units}$$
$$200 \text{ mg} \div 1 \text{ mg} = 200 \text{ Billable Units}$$
Critical Warning: Entering “1” as the unit because you injected “1 vial” or “1 mL” is the single largest source of financial losses for men’s health clinics. If you bill 1 unit of J1071, the insurance provider will pay you for exactly 1 milligram of the drug, resulting in a 99.5% underpayment on the line item.
The table below outlines common clinical doses and how they convert to billable units under J1071:
| Fluid Volume Administered (at 200 mg/mL) | Total Mass (mg) Delivered | Proper J1071 Billable Units |
| 0.25 mL | 50 mg | 50 units |
| 0.50 mL | 100 mg | 100 units |
| 0.75 mL | 150 mg | 150 units |
| 1.00 mL | 200 mg | 200 units |
| 2.00 mL | 400 mg | 400 units |
National Drug Code (NDC) Requirements
A correct HCPCS code and unit count are no longer sufficient on their own. Payers heavily scrutinize the National Drug Code (NDC) to confirm the exact manufacturer, packaging size, and product concentration.
When billing for a 200 mg dose, the NDC format must be converted from the 10-digit format found on the physical box to the standard 11-digit electronic billing format. This is accomplished by adding a leading zero to the appropriate segment where a digit is missing.
Common 11-digit NDC formats for major manufacturers of testosterone cypionate 200 mg/mL include:
- Pfizer (Depo-Testosterone 200 mg/mL, 1 mL vial): 00009-0417-01
- Pfizer (Depo-Testosterone 200 mg/mL, 10 mL vial): 00009-0417-02
- Hikma Pharmaceuticals (Generic 200 mg/mL, 1 mL vial): 00143-9659-01
Always ensure that the NDC listed on the medical claim matches the physical vial pulled from your clinic’s inventory log. An NDC mismatch can result in cross-referencing errors and automated claim rejections.
Pairing J1071 with CPT Administration Codes
HCPCS code J1071 only covers the cost of the actual medication. It does not cover the clinical work, equipment, or time needed to perform the physical injection. To be compensated for the work of injecting the medication, you must report a separate Current Procedural Terminology (CPT) code.
Because testosterone cypionate is an oil-based suspension, it must be delivered deep into muscle tissue. Therefore, you should pair J1071 with the standard therapeutic intramuscular injection code:
- CPT Code 96372: Therapeutic, prophylactic, or diagnostic injection (specify substance or drug); subcutaneous or intramuscular
The Role of Modifier 25
If a patient visits your practice solely to receive their scheduled testosterone injection, you should only bill for the drug (J1071) and the administration (96372).
However, if the provider performs a significant, separately identifiable Evaluation and Management (E/M) service during the same visit—such as reviewing a full hormone panel, adjusting overall treatment plans, or managing multiple comorbidities—you can bill an E/M office visit code (such as 99213 or 99214). In this scenario, you must append Modifier 25 to the E/M code to demonstrate that the assessment went beyond the routine pre-injection evaluation.
Clinical Documentation and Medical Necessity
To ensure reimbursement, clinical documentation must clearly establish medical necessity. Insurance providers rarely approve testosterone claims for vague symptoms like general fatigue or aging without clear clinical data.
Primary Supporting ICD-10-CM Codes
The medical record must link J1071 to an approved diagnostic code indicating a structural or functional hormone deficiency. Common accepted ICD-10-CM codes include:
- E29.1: Testicular hypofunction (includes low testosterone, testicular hypogonadism, and androgen deficiency)
- E23.0: Hypopituitarism (applicable for secondary hypogonadism where pituitary dysfunction causes low testosterone)
- E89.5: Postprocedural testicular hypofunction (for patients who have undergone surgical removal of the testes)
Standard Documentation Requirements
When auditing a claim for J1071, commercial payers and Medicare contractors look for specific markers in the patient’s chart:
Required TRT Insurance Documentation Checklist:
├── Two separate, baseline fasting morning total testosterone blood tests showing levels below standard clinical ranges
├── Documented clinical symptoms (e.g., muscle mass loss, erectile dysfunction, severe fatigue)
├── Clear documentation of the exact injection site (e.g., left gluteus maximus)
├── The exact volume, strength, manufacturer NDC, and lot number of the drug administered
2026 Expected Fee Schedules and Reimbursement
The reimbursement rates for J1071 are tied directly to the Average Sales Price (ASP) updates published quarterly by CMS, alongside adjustments from individual commercial payer fee schedules.
Because the code represents a single milligram, the base unit price looks exceptionally small on paper. The financial viability relies entirely on multiplying that base rate across the full 200-unit spectrum.
| Payer Classification | Average Reimbursement Per Unit (1 mg) | Total Estimated Reimbursement for a 200 mg Dose |
| Medicare Part B (National Average) | $0.041 | $8.20 |
| Major Commercial Payers (UnitedHealthcare, Aetna) | $0.025 – $0.060 | $5.00 – $12.00 |
| Medicaid (State-by-State Average) | $0.020 – $0.035 | $4.00 – $7.00 |
Note: These values represent the payment allowance for the medication itself. The clinical administration fee for CPT 96372 provides additional reimbursement, typically ranging between $25.00 and $45.00 depending on geographic location and contract terms.
Frequently Asked Questions (FAQ)
How many units of J1071 should I report for a single 200 mg injection?
You must report 200 units. Because the billing unit for J1071 is defined as 1 mg, you enter the exact number of milligrams administered to the patient.
Can I bill for testosterone cypionate if the patient self-administers the injection at home?
Generally, no. HCPCS codes starting with “J” are specifically designated for drugs administered “other than oral method” within an outpatient facility or office by a qualified healthcare professional. If a patient self-administers a prescription filled at a retail pharmacy, the pharmacy bills the patient’s pharmacy benefit manager (PBM) using the NDC, and the clinic cannot submit an outpatient medical claim.
What should I do if a commercial insurance plan requires prior authorization for J1071?
Submit a prior authorization request containing the patient’s diagnostic history, clinical notes detailing their symptoms, and copies of two separate fasting morning lab results that show testosterone levels below normal physiological thresholds.
Is there a specific modifier required for wasting medication from a single-dose vial?
If you use a single-dose vial of testosterone cypionate to administer a partial dose (e.g., injecting 150 mg from a 200 mg single-dose vial) and must discard the remaining 50 mg, you can bill for the full 200 mg by appending Modifier JW on a separate line item to document the discarded portion. Do not use this modifier for multi-dose vials.
Additional Resources
For deeper operational details regarding outpatient drug billing and updated ASP fee schedules, review the official resource guides provided by the Centers for Medicare & Medicaid Services (CMS) Medicare Part B Drug Pricing.
Summary
The accurate coding configuration for billing a standard 200 mg dose of testosterone cypionate relies on HCPCS code J1071 reported at exactly 200 billable units, paired with CPT administration code 96372. Proper reimbursement requires clear documentation of clinical hypogonadism, converting the package NDC to an 11-digit billing format, and avoiding old, deleted codes like J1080.
Disclaimer: This article serves as an educational guide for healthcare providers, medical coders, and billers. Coding regulations, fee schedules, and insurance policies change frequently. Always consult the latest official guidelines from the Centers for Medicare & Medicaid Services (CMS), the American Medical Association (AMA), and individual payer policies for active, definitive billing criteria.





