If you are reading this, you probably already know that SMBP (Self-Measured Blood Pressure Monitoring) is a good idea. It helps patients manage hypertension. It helps you keep an eye on them between visits. And yes, it can bring in revenue.
But the coding part? That is where things get messy.
Should you use G2211? Or G0511? Wait, what about 99457? And does Medicare still require 20 minutes of interactive communication?
I have been there. Staring at a claim form. Second-guessing every code. Wondering if I am about to trigger an audit.
This guide is for you. It is not a copy-paste from the CPT manual. It is not a rehash of CMS memos. It is a real, down‑to‑earth walkthrough of how to code SMBP correctly, honestly, and profitably.
What is SMBP and why does coding matter?
SMBP stands for Self-Measured Blood Pressure Monitoring. It is exactly what it sounds like. A patient uses a validated home blood pressure monitor. They take regular readings. They share those readings with you or your team.
But here is the key: SMBP is not just “take your blood pressure at home and call me.” To bill for it, you need structure. You need a clinical purpose. And you need the right codes.
The coding matters because if you get it wrong, you leave money on the table. Or worse, you get a denial. Or a recoupment request. Nobody wants that letter.
Coding SMBP is not about cheating the system. It is about documenting the real work you already do. You review readings. You adjust medications. You call patients when their numbers are scary. That work deserves to be paid.
A quick note on honesty
I will never suggest you bill for work you did not do. That is fraud. This guide assumes you are providing legitimate SMBP services. We are just making sure you get paid correctly for them.
The core SMBP codes you need to know
Before we go deep, here is the cheat sheet.
| Code | What it covers | Who uses it | Typical payment (approx) |
|---|---|---|---|
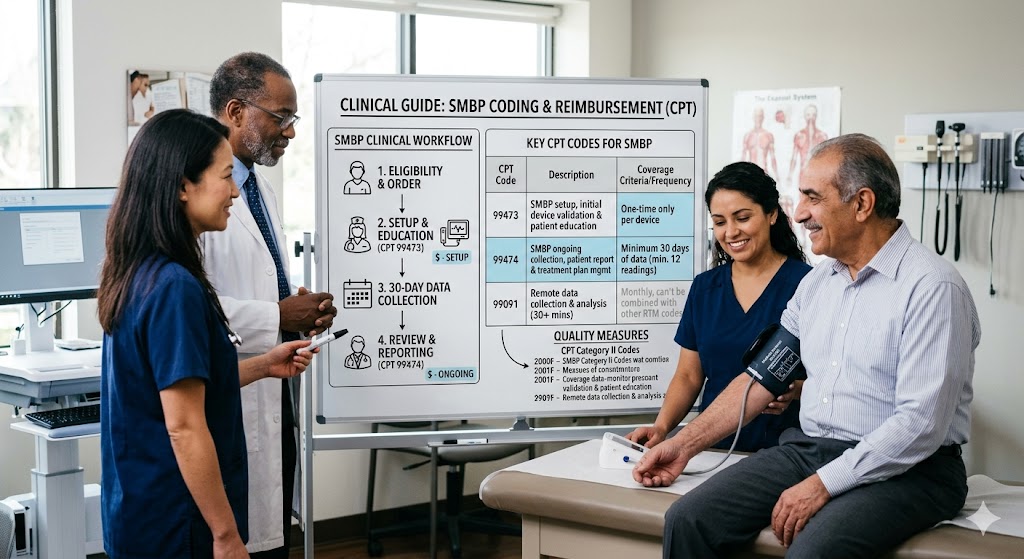
| 99473 | Device setup and patient training (first time) | All payers | $19–$25 |
| 99474 | Reading interpretation and management per 30 days | All payers | $40–$55 |
| G0511 | General care management (includes SMBP for FQHCs/RHCs) | FQHCs, RHCs | Varies by encounter |
| G2211 | Complex visit add‑on (not SMBP‑specific but often paired) | Medicare | ~$16 |
Important note: The prices above are rough Medicare rates. Private payers vary wildly. Always check your local fee schedule.
Now let us break each code down like we are having coffee.
Code 99473: Setting up for success
This is the first step. You cannot bill 99474 unless you have completed 99473 first (with very rare exceptions).
What 99473 includes
- Device selection guidance: Helping the patient pick a validated monitor. Not just any cuff from the drugstore.
- Hands‑on training: Showing the patient how to take readings correctly. Arm position. Time of day. Empty bladder. No talking.
- Initial data upload or log setup: Teaching them how to share readings. That could be an app, a portal, or a paper log.
Who can perform 99473?
A clinical staff member can do this under general supervision. That means a medical assistant, nurse, or even a trained health coach. The physician does not need to be in the room.
How many times can you bill it?
Once per device per patient per lifetime. Unless the patient gets a completely new device (lost, broken, or upgraded). In that case, you can bill again.
Documentation for 99473
Your note should show:
- Date of training
- Type of device (brand/model)
- What you taught (position, timing, frequency)
- Confirmation that the patient understands
- Any barriers identified (poor vision, arthritis, language)
Example note snippet:
*“Patient trained on A&D UA‑767F monitor. Demonstrated proper cuff placement on bare arm, seated position with back supported. Patient returned demonstration correctly. Will record AM readings 3x/week. Log uploaded to patient portal.”*
Code 99474: The monthly monitoring workhorse
This is where the ongoing work lives. You bill 99474 for each 30‑day period of monitoring, interpretation, and management.
What 99474 includes
- Review of at least 12 readings (usually over 30 days)
- Interpretation of patterns
- Clinical management based on those readings (medication changes, lifestyle advice, follow‑up scheduling)
- Communication with the patient (phone, portal, secure message)
Time requirements
There is no strict 20‑minute rule for 99474, unlike some other remote monitoring codes. But you need to show meaningful work. If you spend two minutes forwarding an auto‑report, that is not enough.
How often to bill 99474
Once per calendar month. You can bill it for up to 12 months per condition. After that, you need to reassess if continued monitoring is medically necessary.
Common mistake
Billing 99474 without having a medication change or a management action. Medicare expects you to do something with the data. If all readings are normal and you do nothing, do not bill.
Instead, document your decision.
*“All readings below 130/80. No medication change needed. Patient will continue current lisinopril. Next follow‑up in 3 months.”*
That is still management. “No change” is a clinical decision.
Code G0511: The FQHC and RHC special case
If you work in a Federally Qualified Health Center (FQHC) or a Rural Health Clinic (RHC), your world is different. You do not use 99473 and 99474 directly.
Instead, you use G0511 for general care management that includes SMBP as part of a broader service.
What G0511 covers
G0511 is a bundle. It can include:
- Chronic care management (CCM)
- Remote patient monitoring (RPM)
- Remote physiologic monitoring (RPM)
- And yes, SMBP
But here is the catch. You cannot bill G0511 just for SMBP alone. It must be part of a general care management plan for a patient with one or more chronic conditions.
Documentation for G0511
You need:
- A care plan (written)
- Patient consent (verbal is okay, but document it)
- At least 20 minutes of clinical staff time per month (can be non‑face‑to‑face)
- Involvement of a billing provider
Payment for G0511
Medicare pays a per‑patient per‑month rate. It is lower than billing 99473+99474 separately. But for FQHCs and RHCs, that is the path CMS gives you. Do not try to use 99473/99474. They will deny.
“Our clinic tried billing 99474 for three months before we realized we needed G0511. The denials were painful. Learn from our mistake.”
— Practice manager, rural Nebraska
Code G2211: The complexity add‑on (not SMBP, but relevant)
G2211 is a hot topic. It is an add‑on code for office/outpatient E/M visits (99202–99215) that account for the extra complexity of managing a patient over time.
Why mention it here? Because if you are doing SMBP for a patient with complex hypertension, you may also be doing a higher‑level E/M visit. G2211 can be added to that visit.
But do not add G2211 automatically just because you do SMBP. That is not what it is for.
G2211 is for the relationship. The continuity. The fact that you are the main doctor for a patient with a serious, ongoing condition.
Use it honestly. Or not at all.
Who can bill SMBP codes? (Provider types)
Not everyone can bill every SMBP code. Let us clear this up.
| Provider type | Can bill 99473/99474? | Can bill G0511? | Notes |
|---|---|---|---|
| Physician (MD/DO) | Yes | No (except in FQHC/RHC) | Use standard codes |
| Nurse practitioner (NP) | Yes | No | Same as physician |
| Physician assistant (PA) | Yes | No | Same as physician |
| Clinical nurse specialist (CNS) | Yes | No | Same as physician |
| FQHC/RHC | No | Yes | Must use G0511 |
| Independent lab | No | No | Cannot bill these |
| DME supplier | No | No | Different rules |
If you are a small private practice: Stick with 99473 (once) and 99474 (monthly). Keep it simple.
Payer differences: Medicare vs. commercial vs. Medicaid
This is where many people get lost. The codes are the same, but the rules are not.
Medicare (CMS)
- Follows the rules above closely.
- Requires a diagnostic code like I10 (essential hypertension) or I15 (secondary hypertension).
- Does not require the device to be “connected” (can use paper logs).
- Pays about $19 for 99473 and $48 for 99474 (2025 rates, subject to change).
Commercial payers (UnitedHealthcare, Aetna, Cigna, BCBS)
- Varies enormously.
- Some require the device to be cellular or Bluetooth‑connected.
- Some require a specific platform (e.g., Livongo, Omron).
- Many reimburse less than Medicare.
- A few reimburse more (rare, but happens).
Medicaid
- Highly variable by state.
- Some states do not recognize SMBP codes at all.
- Others require prior authorization.
- Always check your state Medicaid fee schedule.
Self‑pay / cash‑pay
You can always offer SMBP as a cash service. Many patients are willing to pay $30‑50/month for the peace of mind and medication adjustments.
Just provide a good faith estimate. And be transparent.
Setting up a real SMBP workflow (step by step)
Let us move from theory to practice. Here is a workflow that works for a typical primary care practice.
Step 1: Identify candidates
Not every hypertensive patient needs SMBP. Focus on:
- Patients with uncontrolled hypertension (above 140/90)
- Patients with white coat hypertension
- Patients adjusting to new meds
- Pregnant patients with gestational hypertension
- Patients with frequent ER visits for high BP
Step 2: Get consent
Yes, you need consent. Verbal is fine. Document it in the chart.
Script example:
“We would like you to monitor your blood pressure at home. We will review your readings each month and adjust your treatment as needed. Medicare may cover this. You can stop any time. Do you agree?”
Step 3: 99473 – Device training
Schedule a 15‑minute visit (nurse or MA). Teach the patient. Give written instructions. Provide a log or app access.
Step 4: Start the 30‑day clock
Day 1 is the date of training. The patient begins taking readings. Aim for at least 12 readings over 30 days (many practices want 4 per week).
Step 5: 99474 – Monthly review
At least once every 30 days, a clinician (MD, NP, PA) reviews the readings. Document any medication changes or management decisions. Bill 99474.
Step 6: Repeat monthly
Continue until the patient’s BP is stable for 3 months, or until you reach 12 months. Then stop and reassess.
Documentation templates you can steal (I mean, adapt)
I have used these. They work. Tweak them for your EMR.
Template for 99473
text
Copy
Download
**SMBP Device Training** Date: [date] Staff: [name/title] Device: [manufacturer, model] Training provided: - Proper cuff placement (bare arm, at heart level) - Timing (morning before meds, evening before dinner) - Frequency (3x per week) - Recording method (paper log / portal app) Patient return demonstration: [pass / fail / needs repeat] Barriers: [none / arthritis / vision / hearing / language] Plan: [continue, repeat training on next visit] Signed: [staff]
Template for 99474 (monthly)
text
Copy
Download
**SMBP Monthly Review – [month/year]** Readings reviewed: [number] over [days] Average systolic: [X] Average diastolic: [Y] % readings above goal: [Z%] Clinical assessment: [ ] BP at goal – continue current plan [ ] BP above goal – see below [ ] BP below goal (symptomatic) – see below Management actions (check all that apply): [ ] Medication change – [drug, dose, frequency] [ ] Lifestyle counseling – [diet, exercise, salt, alcohol] [ ] Appointment scheduled – [next visit date] [ ] Referral – [cardiology, nephrology] [ ] Patient education – [topic] Communication with patient: [ ] Phone call – [date, duration] [ ] Portal message [ ] In‑person visit Next review due: [date] Billed: 99474
9 common SMBP coding mistakes (and how to avoid them)
After reviewing hundreds of SMBP claims, here is what I see most often.
1. Billing 99474 without a 99473 on file
Medicare’s system looks for a 99473 in the past 12 months. If it is not there, the 99474 denies.
Fix: Do not start billing 99474 until you have completed and billed 99473.
2. Using the wrong place of service
SMBP codes are typically billed with POS 11 (office). If you are training someone remotely (telehealth), check payer rules. Some want POS 02 or 10.
3. Overlapping months
You cannot bill 99474 twice in the same calendar month. For example, billing on February 15 and again on February 28. Wait 30 days.
4. Insufficient readings
Some payers require at least 12 readings in the 30‑day period. If the patient only submits 6, do not bill. Document the failure and try again.
5. No management
Billing 99474 when you did nothing but forward an auto‑report is a compliance risk. Always document a clinical decision, even if that decision is “continue current plan.”
6. Billing for paper logs without a signature
If the patient uses a paper log, you need a way to prove they actually took the readings. A signed log or a verbal confirmation documented in the note is essential.
7. Using G0511 for SMBP only in FQHCs
G0511 requires general care management (e.g., CCM or RPM). SMBP alone does not qualify. Add another chronic condition and care plan.
8. Forgetting to check payer medical policies
I know, reading medical policies is boring. But some payers require prior authorization. Some require a specific device. Spend 10 minutes checking.
9. Not auditing yourself
Every six months, pull a sample of 10 SMBP claims. Check documentation against payment. If you find patterns of error, fix your workflow.
How much money are we talking about? (Realistic revenue)
Let us do the math. Assume Medicare rates (2025 estimates).
Per patient, first month:
- 99473: $19
- 99474: $48
- Total: $67
Months 2 through 12 (each):
- 99474: $48
- Total per month: $48
Annual revenue per patient (if monitored for 12 months):
- First month: $67
- Next 11 months: 11 x $48 = $528
- Total: $595 per patient per year
Now multiply that by 50 patients. That is nearly $30,000 in additional revenue. For work you are probably already doing.
But remember: private payers may pay less. Staff time costs money. Device costs may be yours or the patient’s. Net revenue is lower.
SMBP and value‑based care
Here is something many coding guides skip. SMBP is not just about fee‑for‑service. It helps in value‑based contracts too.
If you are in a Medicare Shared Savings Program (MSSP) ACO, or a commercial ACO, better BP control improves your quality scores. Those scores affect shared savings payments.
Example: The CMS ACO REACH program includes hypertension control as a quality measure. SMBP is one of the best ways to improve that measure.
So even if insurance underpays for 99474, the ACO bonus may more than make up for it.
Patient eligibility checklist
Use this before starting SMBP billing.
- Patient has hypertension (ICD‑10 I10 or I15)
- Patient is able and willing to take readings
- Patient has a validated home monitor (not a wrist cuff from Amazon)
- Patient has a way to share readings (portal, app, phone, fax, paper)
- Patient has not used 99473 in the last 12 months (unless new device)
- No active denial or audit flag for SMBP codes
- Verbal consent documented
Device requirements: What CMS actually says
CMS does not require a specific brand. But they do require a validated device. The patient can buy it themselves, or you can provide it.
Validated devices are listed on:
- ValidateBP.org (from the American Medical Association)
- STRIDE BP (international validation)
Do not recommend unvalidated devices. If a patient shows up with a wrist cuff that is not validated, document that you counseled them on proper device selection. Bill 99473 anyway for the training. The training still happened.
Can you bill SMBP for patients in nursing homes?
Yes, but with caution. If the patient is in a skilled nursing facility (SNF) and under a Part A stay, SMBP is bundled into the facility payment. You cannot bill separately.
If the patient is in long‑term care (non‑Part A), you can bill SMBP the same way as in the community.
Telehealth and SMBP: A confusing relationship
Many practices want to do the 99473 training via video call. Is that allowed?
- Medicare: Yes, for 99473. Use POS 02 (telehealth) and modifier 95. But check your local MAC. Some still prefer in‑person.
- Commercial payers: Mostly yes, but some require modifier GT or 93. Check each plan.
For 99474, it is not a “visit” per se. It is management work. You can do it from anywhere. No modifier needed.
What about using unlicensed staff?
You can use medical assistants (MAs) for 99473 training. That is fine.
You cannot use MAs to interpret readings or make medication changes. That is the clinician’s job (MD, NP, PA).
For 99474, the interpreting provider must be a licensed clinician. The MA can help by logging data, but the clinical decision is yours.
When NOT to bill SMBP
Honesty time. Do not bill SMBP in these situations:
- The patient does not have hypertension (you are just “checking” for fun)
- The patient takes readings but you never look at them
- The patient is in the hospital (inpatient)
- The patient is in a SNF under Medicare Part A
- You have not seen the patient in person in the last 12 months (for new starts)
- The patient cannot or will not share readings (no data = no bill)
Medicare Advantage plans (Part C)
Medicare Advantage plans often follow CMS rules for SMBP. But not always.
Some MA plans:
- Require prior authorization
- Use different codes (like G2212 for complex monitoring)
- Have lower reimbursement
- Bundle SMBP into the monthly capitation payment
Call the plan’s provider line. Ask: “Do you cover 99473 and 99474? Any special requirements?” Get a reference number for the call.
State‑specific Medicaid oddities
I cannot list all 50 states, but here are patterns.
- California (Medi‑Cal): Does not separately reimburse 99473/99474 as of 2025. Use E&M codes.
- Texas (THSteps for kids): No SMBP codes.
- New York (Medicaid): Reimburses 99474 but requires 99473 within previous 6 months.
- Florida: Reimburses at 80% of Medicare rate.
Golden rule: Search “[your state] Medicaid fee schedule SMBP”. If nothing comes up, call them.
How to handle patient‑owned devices
Many patients already have a blood pressure cuff. They come to you and say, “Can I use my own device?”
Yes. You can still bill 99473 for the training. You do not need to sell them a new device.
Document: “Patient has validated device (Omron Series 10). Training provided on proper use. Device compatible with our log.”
That is compliant.
What happens if you lose the patient log?
It happens. The app crashes. The patient forgets their password. The paper log gets wet.
Do not bill 99474 for that month. Instead, document: “Unable to retrieve readings due to technical issue. Attempted retrieval on [dates]. Will restart monitoring next month.”
Then either repeat 99473 (if it is a new device or new platform) or just start fresh the next month without billing.
Annual wellness visits and SMBP
Many practices integrate SMBP training into the Annual Wellness Visit (AWV). Good idea. But careful.
The AWV (G0438 or G0439) includes a lot. SMBP training is not part of the standard AWV. You can add it, but you must document it separately. And you can bill 99473 on the same day as the AWV. No modifier needed for Medicare.
Example: Patient comes for AWV. After the AWV is complete, MA spends 10 minutes on SMBP training. Bill G0438 (AWV) and 99473. Both get paid.
How to fight a denial (step by simple step)
Denials happen. Do not panic. Do this.
Step 1: Read the denial reason on your remittance advice (RA). Common reasons:
- N290 (missing 99473)
- N362 (missing medical necessity)
- CO 234 (payer does not cover this code)
Step 2: Check your documentation. Do you have the consent note? The reading log? The management action?
Step 3: If documentation is good, appeal. Write a one‑page letter. Include:
- Patient name, ID, date of service
- Code denied
- Why it is correct (cite CMS manual section if needed)
- Attach your documentation
Step 4: If the denial was your error (e.g., forgot to bill 99473 first), do not appeal. Write it off. Fix your process.
Step 5: If the payer denies all SMBP codes as “not covered,” add them to your list of payers where you do not offer SMBP billing. Offer it as a cash service instead.
SMBP for pregnancy and postpartum hypertension
This is a growing area. Gestational hypertension and preeclampsia are dangerous. SMBP helps.
Medicare of course does not cover pregnancy (except for disabled or over‑65). But commercial payers increasingly cover SMBP for pregnant patients.
Coding is the same: 99473 + 99474. ICD‑10 codes change: O13 (gestational hypertension) or O14 (preeclampsia).
Important: Some payers require a specific postpartum monitoring period (up to 6 weeks after delivery). After that, switch to chronic hypertension codes if needed.
Future of SMBP coding: What to watch
CMS updates codes every year. Here is what is coming.
- Integration with SDOH (social determinants of health): New codes for addressing food insecurity, housing, transportation. SMBP may bundle with those.
- AI‑assisted interpretation: Not yet coded separately, but coming.
- Hypertension‑only remote monitoring bundles: Some specialty societies are asking for a single SMBP monthly code (no separate training code).
Check the CPT manual each fall. Do not assume last year’s rules still apply.
Sample dialogue for talking to patients about SMBP costs
Patients may worry about the bill. Be upfront.
“This service is usually covered by Medicare and many insurance plans. You might have a small copay, like you do for an office visit. I cannot guarantee coverage, but we will check for you first. Would you like to proceed?”
If the patient is self‑pay:
“We charge $40 per month for the monitoring service. The device you buy yourself, about $40‑60. If that is too much, we can work something out.”
Quick reference: SMBP coding decision tree
Ask these questions in order.
- Is the patient in an FQHC or RHC?
- Yes → Use G0511 (with general care management)
- No → Go to question 2
- Has the patient completed 99473 in the last 12 months?
- No → Bill 99473 first, then start monthly 99474
- Yes → Go to question 3
- Is this a new 30‑day period since last 99474?
- Yes → Bill 99474
- No → Wait
- Did you make a clinical management decision?
- Yes → Good, document it
- No → Do not bill
Final workflow checklist (print this)
Before starting SMBP for a patient:
- Identify patient with uncontrolled or problematic hypertension
- Obtain verbal consent (document)
- Provide or confirm validated device
- Schedule 99473 training (15 min with MA/nurse)
- Bill 99473
Each month:
- Ensure at least 12 readings available
- Clinician reviews readings
- Document management action (including “no change”)
- Bill 99474
- Set reminder for next month
Every 6 months:
- Audit 5-10 SMBP charts
- Check for missing documentation
- Check payer policy updates
At 12 months:
- Reassess need for continued monitoring
- If no longer needed, stop billing
- If still needed, continue with 99474 (no repeat 99473 unless new device)
Conclusion (three lines)
SMBP coding does not have to be a headache. Stick to 99473 for initial training, then 99474 monthly. Document your clinical decisions honestly, check payer rules, and you will get paid for work you already do.
Frequently Asked Questions (FAQ)
1. Can I bill 99473 and 99474 on the same day?
Yes, but only on the very first day. After that, they are separate. You cannot bill 99474 on the same day as another 99474.
2. Do I need a special EMR module for SMBP?
No. You can use paper logs and standard EMR notes. Connected devices are nice but not required for Medicare.
3. What if the patient forgets to take readings most weeks?
Do not bill for that month. Document coaching. If the patient remains non‑adherent, discontinue SMBP billing.
4. Can I bill SMBP for a patient I see only via telehealth?
Yes, but you need an in‑person relationship established first. For Medicare, you must have seen the patient in person within the last 12 months before starting SMBP.
5. What modifier do I use for SMBP?
Generally none. Use modifier 95 for telehealth training (99473 via video). Use modifier 25 for same‑day E/M visits if the E/M is separate and significant.
6. Is SMBP considered “incident to” billing?
Yes, if performed by clinical staff under general supervision. The billing provider must have seen the patient at least once for the condition.
7. Does the patient have to buy the device from me?
No. Never require that. That could violate anti‑kickback rules. The patient can buy from any source.
8. Can I bill G0511 and 99474 for the same patient in the same month?
No. Choose one. FQHCs/RHCs use G0511. Everyone else uses 99474.
9. What ICD‑10 code should I use?
Primary: I10 (essential hypertension). Secondary: I15.0 (renovascular), I15.8 (other secondary), or Z01.89 (encounter for other specified special exam) if screening.
10. How long do I keep SMBP documentation?
Same as any medical record. At least 7 years. Longer if required by your state or payer.
Additional resource
For the most up‑to‑date list of validated blood pressure monitors and detailed billing examples from the American Medical Association, visit:
ValidateBP.org
This is a free, reliable, and non‑commercial resource run by the AMA and the American Heart Association.
Disclaimer
This article is for educational purposes only. Coding rules change frequently and vary by payer, state, and individual patient circumstances. Always verify with your local Medicare Administrative Contractor (MAC), commercial payer policies, and your compliance officer before billing. The author and publisher assume no liability for denied claims, audits, or any other consequences arising from the use of this information. When in doubt, consult a certified professional coder or healthcare attorney.





