In the high-stakes world of surgical coding, few areas demand as much precision, anatomical knowledge, and attention to detail as craniomaxillofacial trauma. A zygomaticomaxillary complex (ZMC) fracture, often colloquially called a “tripod” or “malar” fracture, is a common yet intricate injury resulting from significant facial trauma. For the medical coder, accurately translating the complex surgical repair of a ZMC fracture into the correct Current Procedural Terminology (CPT®) codes is a critical task. It is a task that sits at the intersection of clinical medicine, administrative compliance, and financial stability. An accurately coded claim ensures appropriate reimbursement for the surgeon’s skill and time, reflects the true complexity of the patient’s condition, and, most importantly, creates a clean and defensible medical record. Conversely, incorrect coding can lead to claim denials, delayed payments, audits, and potential legal ramifications.
This article serves as an exhaustive guide for coders, billers, surgeons, and healthcare administrators. We will embark on a detailed journey from the foundational anatomy of the ZMC, through the clinical pathways of diagnosis and treatment, and into the nuanced world of CPT codes 21355, 21365, 21385, and their companions. We will dissect common clinical scenarios, clarify the use of essential modifiers, underscore the non-negotiable importance of documentation, and outline strategies for maintaining compliance in an ever-evolving regulatory landscape. Our goal is to transform the complexity of ZMC fracture coding from a daunting challenge into a mastered skill.
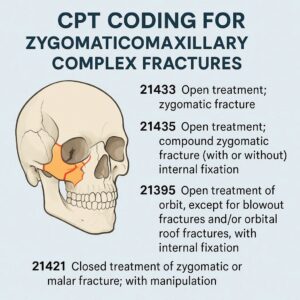
CPT Coding for Zygomaticomaxillary Complex Fractures
Table of Contents
Toggle2. Anatomy 101: Deconstructing the Zygomaticomaxillary Complex
To code effectively, one must first understand what is being repaired. The zygomatic bone, or cheekbone, is a key aesthetic and functional pillar of the midface. It provides the prominent contour of the cheek, forms the lateral wall and floor of the orbit, and contributes to the lateral portion of the orbital rim. The term “Zygomaticomaxillary Complex” is used because a fracture rarely involves the zygomatic bone in isolation. Instead, the force of trauma typically separates the zygoma at its four key sutural attachments, creating a fracture “complex”:
-
Zygomaticofrontal (ZF) Sutures: The attachment point of the zygoma to the frontal bone at the lateral aspect of the eyebrow.
-
Zygomaticomaxillary (ZM) Buttress: The critical vertical support where the zygoma articulates with the maxilla (upper jaw). This is often comminuted (shattered into multiple pieces).
-
Zygomaticotemporal (ZT) Sutures: The connection along the zygomatic arch, which extends posteriorly towards the temporal bone.
-
Zygomaticosphenoid (ZS) Sutures: The articulation between the zygoma and the greater wing of the sphenoid bone deep within the orbit.
A true ZMC fracture involves disruptions at all four of these points. The bone itself often remains intact but is displaced as a single unit. Understanding this anatomy is paramount because CPT codes are frequently based on the number of these key areas that require surgical repair and fixation.
-
Figure 1: Anatomical Diagram of the ZMC: (A detailed illustration showing the zygomatic bone and its four sutural attachments: ZF, ZM, ZT, and ZS. The diagram would highlight the “tripod” concept, though it’s technically a tetrapod.)
3. The Clinical Picture: Mechanisms of Injury, Diagnosis, and Classification
ZMC fractures are typically the result of high-impact trauma. Common mechanisms include:
-
Assaults (fisticuffs, blunt objects)
-
Motor vehicle accidents (MVAs)
-
Sports injuries
-
Falls
Patients present with classic signs and symptoms: flattening of the cheek prominence, periorbital ecchymosis (black eye), subconjunctival hemorrhage, diplopia (double vision) due to orbital volume change or muscle entrapment, trismus (difficulty opening the mouth) due to impingement on the coronoid process of the mandible, and numbness in the cheek, upper lip, and teeth due to injury to the infraorbital nerve.
Diagnosis begins with a physical exam but is confirmed radiologically. A computed tomography (CT) scan with thin-cut axial and coronal views is the gold standard. It provides a 3D understanding of the fracture pattern, the degree of displacement, and rotation, and identifies any associated orbital floor fractures.
Surgeons classify ZMC fractures to guide treatment. Common classifications include:
-
Knight and North: Based on the pattern seen on plain X-rays (less used today).
-
Zingg Classification:
-
Type A: Incomplete fracture, one pillar involved.
-
Type B: Complete monoblock fracture (all four sutures disrupted).
-
Type C: Complex comminuted fractures (multi-fragmentary).
-
The treatment plan—closed versus open reduction—depends on factors like displacement, functional impairment (diplopia, trismus), and aesthetic concerns.
4. The CPT® Coding Ecosystem: A Primer on Fundamentals
The CPT code set, maintained by the American Medical Association (AMA), is a uniform language for describing medical, surgical, and diagnostic services. Codes for fracture care are found in the Musculoskeletal System section, specifically under “Head” (CPT codes 21355-21497). Key concepts for ZMC coding include:
-
Global Period: Most fracture care codes have a 90-day global period. This means the reimbursement for the code includes all related preoperative, intraoperative, and postoperative care for 90 days following the surgery. Follow-up visits, minor wound care, and routine dressing changes during this period are not separately billable.
-
Bundling: CPT and National Correct Coding Initiative (NCCI) edits define which procedures are considered integral to a primary service and are therefore “bundled” and not separately reportable.
-
Medical Necessity: The cornerstone of all coding. The diagnosis code (ICD-10-CM) must justify the procedure performed (CPT code).
5. Deep Dive into Specific CPT Codes for ZMC Fractures
The choice of code hinges on two primary factors: the method of treatment (closed vs. open reduction) and the number of fixation points (if open reduction is performed).
5.1. Closed Treatment Codes (21355, 21356, 21360)
Closed treatment involves manipulating the fracture into alignment without making an open incision to visualize the fracture fragments.
-
CPT 21355: Closed treatment of zygomatic fracture; without manipulation.
-
Use Case: For a stable, non-displaced or minimally displaced fracture that requires no active reduction—only symptomatic care like observation, ice, and soft diet.
-
-
CPT 21356: Closed treatment of zygomatic fracture; with manipulation.
-
Use Case: The surgeon performs an manual reduction, such as a Gilles approach (placing an elevator behind the zygoma, typically via a temporal incision) to “pop” the bone back into place. No internal fixation is placed, and the reduction is stabilized by the surrounding soft tissues alone.
-
-
CPT 21360: Percutaneous treatment of zygomatic fracture, with manipulation.
-
Use Case: This is a grey area. It involves manipulation, and while it is “percutaneous” (through the skin), it may involve passing wires or pins to help stabilize the reduction (e.g., a Carroll-Girard screw). If any form of internal fixation is placed that remains after surgery, it typically crosses into open treatment.
-
5.2. Open Treatment with Internal Fixation Codes (21365, 21366, 21385, 21395)
Open treatment (ORIF) involves surgical exposure of the fracture site(s), direct visualization of the fragments, anatomic reduction, and application of internal fixation (e.g., titanium plates and screws).
-
CPT 21365: Open treatment of zygomatic fracture; without internal fixation.
-
Use Case: Extremely rare. This would involve opening the fracture, reducing it, and then stabilizing it without plates or screws, perhaps with a external fixation device.
-
-
CPT 21366: Open treatment of zygomatic fracture; with internal fixation.
-
Use Case: The workhorse code for most simple ZMC ORIFs. This code is used when the fracture is exposed, reduced, and fixated at one or two points. For example, fixation at the zygomaticomaxillary buttress and the zygomaticofrontal suture.
-
-
CPT 21385: Open treatment of craniofacial separation…
-
Note: This code is NOT for a typical ZMC fracture. It is for a Le Fort III type pattern or true craniofacial dysfunction. Using this for a standard ZMC fracture is incorrect and would be considered upcoding.
-
-
CPT 21395: Open treatment of zygomatic fracture, with internal fixation; of tripod fracture, with multiple surgical approaches.
-
Use Case: This is a comprehensive code used when the ZMC fracture is fixated at three or more points and requires multiple surgical approaches (e.g., a lateral brow incision for the ZF suture, a transconjunctival or subciliary incision for the infraorbital rim/orbital floor, and a intraoral (gingivobuccal sulcus) incision for the ZM buttress). This code is valued higher than 21366 because of the increased complexity, time, and work involved.
-
Summary of Primary ZMC Fracture CPT Codes
| CPT Code | Procedure Description | Key Clinical Application | Number of Fixation Points |
|---|---|---|---|
| 21355 | Closed treatment without manipulation | Stable, non-displaced fracture | N/A |
| 21356 | Closed treatment with manipulation | Reduced manually (e.g., Gilles lift), no fixation | N/A |
| 21360 | Percutaneous treatment with manipulation | Reduced percutaneously, may have temporary pin | N/A |
| 21365 | Open treatment without internal fixation | Rarely used | N/A |
| 21366 | Open treatment with internal fixation | Simple ORIF: Fixation at 1 or 2 points | 1-2 |
| 21395 | Open treatment of tripod fracture, multiple approaches | Complex ORIF: Fixation at 3 or more points | 3+ |
5.3. Bone Grafting and Other Associated Procedures (21210, 21215, 21141, 21142, 21143)
ZMC fractures, especially those with comminution or orbital involvement, often require ancillary procedures.
-
Orbital Floor Repair: If the orbital floor is fractured and requires repair, this is coded separately. This is a critical distinction.
-
CPT 21385: Open treatment of orbital floor blowout fracture; periorbital approach. (This is the correct code for a pure orbital floor fracture, not 21385 for craniofacial separation).
-
CPT 21386: …with bone graft (includes obtaining graft).
-
CPT 21387: …with implant.
-
-
Bone Grafting: If a bone graft is used to reconstruct a comminuted area (e.g., the ZM buttress), it may be separately reportable.
-
CPT 21210: Graft, bone; nasal, maxillary or malar areas (includes obtaining graft).
-
CPT 21215: Graft, bone; mandible (includes obtaining graft).
-
-
Reduction of Orbital Fracture: There are specific codes for the isolated reduction of orbital fractures, which are distinct from ZMC codes.
-
CPT 21141 (without graft), 21142 (with graft), 21143 (with implant).
-
Coding Alert: NCCI edits often bundle bone graft codes (21210) with the primary fracture repair code (21366, 21395). However, if the graft is for a separate and distinct defect—such as a significant segmental bone loss in the maxilla that is not part of the fracture line being plated—it may be reported with a modifier (e.g., Modifier 59). Documentation must clearly support the medical necessity of a separate graft.
6. The Art of Code Selection: Navigating Clinical Scenarios
Let’s apply the codes to real-world operative reports.
Scenario 1: The Simple ZMC ORIF
-
Op Note Findings: Displaced left ZMC fracture.
-
Procedure: “A lateral brow incision was made to expose the ZF suture. A gingivobuccal sulcus incision was made to expose the ZM buttress. The fracture was reduced. A 4-hole L-plate was placed at the ZF suture and a 5-hole L-plate was placed at the ZM buttress. Incisions closed in layers.”
-
Correct Coding: 21366. Fixation was performed at two points (ZF and ZM).
Scenario 2: The Complex ZMC ORIF with Orbital Floor Repair
-
Op Note Findings: Comminuted right ZMC fracture with a displaced orbital floor fracture and diplopia.
-
Procedure: “Lateral brow incision (ZF), transconjunctival incision with cantholysis (infraorbital rim and orbital floor), and intraoral incision (ZM). The ZMC was reduced and plated at the ZF, infraorbital rim, and ZM buttress. The orbital floor fracture was noted to be comminuted with herniation of orbital contents. It was reduced, and a porous polyethylene implant was placed to reconstruct the orbital floor.”
-
Correct Coding: 21395 (for the ZMC ORIF at three points: ZF, IO rim, ZM) + 21387 (for the orbital floor repair with implant). A modifier, likely Modifier 51 (Multiple Procedures), would be appended to 21387 because it is a separate procedure performed in the same session. Documentation must clearly link the orbital floor repair to the functional deficit (diplopia).
Scenario 3: The Misclassified Case
-
Op Note Findings: “ZMC tripod fracture.”
-
Procedure: “Open reduction and internal fixation of zygomaticomaxillary complex fracture via lateral brow and intraoral approaches. Plates applied at zygomaticofrontal suture and zygomaticomaxillary buttress.”
-
Incorrect Coding: 21395. Although the narrative says “tripod,” the procedure only describes fixation at two points. The fracture may be a “tripod” by nature, but the treatment was a two-point fixation.
-
Correct Coding: 21366. The code is based on the work performed, not the name of the fracture.
7. Modifiers and Multiple Procedures: Avoiding Bundling Pitfalls
Modifiers are essential to provide payers with additional information about the circumstances of a service.
-
Modifier 51 (Multiple Procedures): Indicates that multiple procedures were performed during the same surgical session. The primary procedure (usually the highest-valued) is listed first without a modifier. Subsequent procedures are appended with Modifier 51. *e.g., 21395, 21387-51.*
-
Modifier 59 (Distinct Procedural Service): Used to indicate that a procedure or service was distinct or independent from other services performed on the same day. It is often used to bypass NCCI bundling edits when procedures are performed on anatomically distinct sites. For example, if a surgeon repairs a ZMC fracture (21366) and also repairs a separate nasal fracture (21336) on the same day, Modifier 59 would be appended to the secondary procedure to indicate it was distinct: *21366, 21336-59*.
-
Modifier 22 (Increased Procedural Services): Used when the work required to provide a service is substantially greater than typically required. This is rarely granted and requires extensive documentation. An example might be a severely comminuted ZMC fracture in a polytrauma patient that took extraordinary time and effort to reconstruct.
-
Modifier 50 (Bilateral Procedure): While rare for trauma, if a patient sustained bilateral ZMC fractures and both were repaired in the same session, you would report the code once with Modifier 50. *e.g., 21366-50.*
8. ICD-10-CM Coordination: The Foundation of Medical Necessity
The ICD-10-CM code tells the “why” behind the CPT code’s “what.” Using the most specific diagnosis code is crucial.
-
S02.4XXA: Fracture of malar, maxillary and zygomatic bones, initial encounter for closed fracture.
-
S02.4XXB: …initial encounter for open fracture.
-
S02.401A: Fracture of malar, maxillary and zygomatic bones, right side, initial encounter for closed fracture.
-
S02.402A: …left side…
-
S02.409A: …unspecified side…
-
S05.10XA: Injury of optic nerve, right eye, initial encounter. (This would be used in addition to the fracture code if applicable to justify orbital exploration).
-
H53.2: Diplopia. (A functional diagnosis that justifies orbital floor repair).
Always use the 7th character (A, D, S) to indicate the encounter status (initial, subsequent, sequela).
9. Documentation is King: What Surgeons Must Record for Optimal Coding
The operative report is the coder’s only source of truth. Vague notes lead to downcoding or denials. Surgeons should document:
-
Preoperative Diagnosis: e.g., “Displaced left ZMC fracture with orbital floor involvement and diplopia.”
-
Postoperative Diagnosis: Should be specific.
-
Procedure(s) Performed: A clear list.
-
Detailed Description:
-
Incisions: List all surgical approaches (e.g., “lateral brow incision,” “transconjunctival incision with lateral canthotomy,” “gingivobuccal sulcus incision”).
-
Findings: Describe the fracture’s location, displacement, comminution, and involvement of other structures (e.g., “orbital floor defect approximately 2.0 x 1.5 cm with herniation of periorbital fat”).
-
Reduction: “The zygomatic complex was mobilized and reduced into anatomic position.”
-
Fixation: Be specific! “A 4-hole titanium miniplate was placed at the zygomaticofrontal suture. A 6-hole titanium miniplate was placed at the infraorbital rim. A 5-hole L-plate was placed at the zygomaticomaxillary buttress.” This directly supports 21395.
-
Ancillary Procedures: “The orbital floor was reconstructed with a preformed 0.4mm porous polyethylene implant.” (Supports 21387).
-
-
Implants: Note the type and size of any plates, screws, or grafts used.
10. Audit and Compliance: Protecting Your Practice
Regular internal audits are a best practice. Review a sample of ZMC fracture cases to ensure:
-
The CPT code matches the number of fixation points documented.
-
Separate procedures (like orbital floor repair) are supported by detailed documentation and appropriately modified.
-
Diagnosis codes are specific and linked correctly to justify medical necessity.
-
Modifier use is consistent with NCCI and payer guidelines.
This proactive approach identifies errors before an external auditor does and helps educate both coders and surgeons.
11. The Future of Craniomaxillofacial Coding: Trends and Technologies
The field is evolving, and coding must keep pace.
-
Virtual Surgical Planning (VSP) & 3D Printing: Surgeons use CT data to pre-plan osteotomies and print custom guides and plates. While there is no specific CPT code for VSP yet, it is often reported with an unlisted procedure code (e.g., 21199) or covered under the primary procedure. This is an area to watch for new code development.
-
Intraoperative Navigation: The use of GPS-like systems to guide reduction. This is also typically considered part of the global service but may be billable in very complex cases with modifier 22 and strong documentation of its necessity.
-
Endoscopic Assistance: Some surgeons use endoscopes for approaches to the orbital floor or zygomatic arch. Again, this is usually bundled but represents increasing technological complexity.
12. Conclusion
Accurate coding for ZMC fractures is a meticulous process rooted in a deep understanding of anatomy, surgical technique, and CPT guidelines. The critical distinction lies in identifying the number of fixation points to choose between 21366 and 21395, while diligently reporting separately identifiable procedures like orbital floor repair. Impeccable documentation is the non-negotiable foundation that supports code selection, ensures compliance, and secures appropriate reimbursement for the complex surgical care provided. Continuous education and internal auditing are the best defenses against the risks of denials and audits in this specialized field.
13. Frequently Asked Questions (FAQs)
Q1: Can I report code 21395 if the surgeon makes three incisions but only places plates at two of them?
A: No. Code selection is based on the number of sites where internal fixation is applied, not the number of incisions made. If an incision is used only for visualization or reduction but no plate is placed at that site, it does not count toward the “multiple surgical approaches” required for 21395. 21366 would be appropriate.
Q2: How do I code for the repair of a isolated zygomatic arch fracture?
A: An isolated fracture of the arch (without ZMC involvement) is coded differently. Use CPT 21440 (Closed treatment of zygomatic arch fracture) or CPT 21445 (Open treatment of zygomatic arch fracture).
Q3: Is the placement of a Carroll-Girard screw for reduction reported separately?
A: No. The use of a screw for leverage during reduction is considered an integral part of the fracture manipulation and is included in the reduction code (21356, 21360, or the open treatment codes).
Q4: What is the correct coding for a “tripod” fracture that is only treated at one point?
A: You code based on the treatment provided, not the fracture name. If the surgeon only places fixation at one point (e.g., only at the ZM buttress believing it is sufficient for stability), you would report 21366. The documentation must explain the rationale for this approach.
14. Additional Resources
-
American Medical Association (AMA): For the official CPT® code book and updates. https://www.ama-assn.org/
-
Centers for Medicare & Medicaid Services (CMS): For National Correct Coding Initiative (NCCI) edits and Medicare-specific guidance. https://www.cms.gov/
-
American Academy of Professional Coders (AAPC): For ongoing education, certifications, and coding forums. https://www.aapc.com/
-
American Society of Maxillofacial Surgeons (ASMS): Often provides clinical perspectives that can inform coding understanding. https://www.maxface.org/
-
Local Carrier Advisory Committees (LCAC): Check for your local Medicare administrative contractor’s (MAC’s) specific policies regarding fracture care coding.
Date: September 14, 2025
Author: The Medical Coding Specialist Team
Disclaimer: This article is for informational and educational purposes only. It is not a substitute for the independent medical judgment of a qualified healthcare provider. CPT® codes, descriptions, and other data are copyright of the American Medical Association (AMA). All rights reserved. Fee schedules, relative value units, conversion factors, and/or related components are not assigned by the AMA and are not part of CPT. The responsibility for content, including any inconsistencies, lies with the author and not with the AMA. Always consult the most current, official AMA CPT® code books and payer-specific guidelines for accurate coding and billing. The information herein does not constitute legal or coding advice.





