If you have ever stared at a surgical report for a carotid angiogram and felt unsure which code to pick, you are not alone.
Few areas in interventional radiology billing cause as much confusion as the carotid artery family of codes. The difference between a diagnostic study and a diagnostic study followed by intervention changes everything. So does the approach—whether the doctor goes through the aortic arch or selectively catheterizes the vessel.
This guide walks you through everything you need to know about the correct CPT code for a carotid angiogram. We will keep the language simple, the examples practical, and the advice honest.
Let us start with the most important fact you need today.
CPT Code for Carotid Angiogram
What Is a Carotid Angiogram?
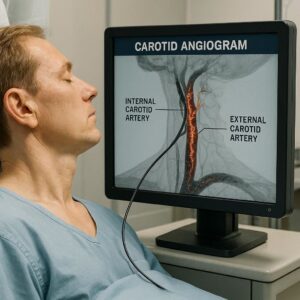
A carotid angiogram is an imaging test that looks at the carotid arteries. These are the main blood vessels on each side of your neck. They carry blood from your heart to your brain.
During the procedure, a radiologist or cardiologist injects a contrast dye through a small tube called a catheter. Then, they take X-ray images. The dye makes the blood vessels visible. This helps the doctor see blockages, narrowing, aneurysms, or tears in the artery wall.
Think of it like a road map for the blood vessels leading to the brain.
Doctors usually order this test when a patient has symptoms of a stroke or transient ischemic attack (TIA). They also use it to plan for surgery or stenting.
Now, let us talk about the numbers that matter for billing.
The Primary CPT Code for Carotid Angiogram
The most common CPT code you will use for a carotid angiogram depends on what the doctor did during the procedure. You cannot just pick one code for every case. You have to read the note.
Here are the main codes for diagnostic carotid angiography:
-
36221 – Non-selective catheter placement, first order thoracic arch branch, with angiography
-
36222 – Selective catheter placement, common carotid or innominate artery, with angiography
-
36223 – Selective catheter placement, internal carotid artery, with angiography
-
36224 – Selective catheter placement, external carotid artery, with angiography
-
36225 – Selective catheter placement, vertebral artery, with angiography
-
36226 – Selective catheter placement, subclavian artery, with angiography
-
36227 – Selective catheter placement, internal carotid artery, with angiography and intervention
Wait—that last one includes intervention. We will get to that soon.
For a pure diagnostic carotid angiogram, 36223 (selective internal carotid angiography) is often the star of the show. But do not assume that. The doctor must document selective catheterization of the vessel of interest.
Breaking Down the Difference
Let me make this very simple.
| Code | What It Means | Typical Use |
|---|---|---|
| 36221 | Non-selective arch study | Looking at multiple vessels from a single catheter position |
| 36222 | Selective common carotid | Imaging the main carotid trunk before it divides |
| 36223 | Selective internal carotid | Imaging the vessel that goes directly to the brain |
| 36224 | Selective external carotid | Imaging branches that supply the face and scalp |
| 36225 | Selective vertebral | Imaging the vessel that supplies the back of the brain |
| 36226 | Selective subclavian | Imaging the vessel under the collarbone |
You cannot bill two selective codes for the same vessel family on the same side in one session unless the doctor documents a separate clinical reason. The National Correct Coding Initiative (NCCI) bundles many of these together.
When to Use Code 36223 (The Most Common Code)
Let us focus on 36223 because it is the workhorse code for carotid angiograms.
You use 36223 when the doctor selectively places a catheter into the internal carotid artery. That is the vessel that supplies most of the blood to your brain. Then, they inject contrast and take images.
The documentation must show:
-
Selective catheterization of the internal carotid artery
-
Injection of contrast
-
Imaging of the vessel
-
A medical necessity reason (like suspected stenosis or prior TIA)
Here is an example from a real report:
*”Using a 5-French diagnostic catheter, I selectively engaged the right internal carotid artery. Angiography was performed in AP and lateral projections. There was 60% stenosis at the origin.”*
That is 36223 for the right side.
But what if the doctor does both sides? Good question.
Bilateral Carotid Angiogram Coding
If the doctor selectively catheterizes both the right and left internal carotid arteries, you have two options.
-
Modifier 50 (Bilateral procedure) attached to one unit of 36223
-
Two units of 36223 with modifier 59 or XS on the second
Most payers prefer modifier 50. But check your local MAC. Some commercial insurers want two line items with modifier 59.
You cannot assume bilateral means double payment. Many payers reduce the second side by 50%.
Always check the medical policy.
What About Non-Selective Studies? (Code 36221)
Sometimes the doctor does not go deep into the internal carotid. They leave the catheter in the aortic arch or the origin of the brachiocephalic artery. Then, they inject contrast and let it flow downstream. That is a non-selective study.
You use 36221 for that.
But here is the catch. Most payers consider a non-selective arch study as a lesser service. If the doctor later does a selective study, you cannot bill both. The selective code includes the non-selective work.
NCCI edits bundle 36221 into 36222, 36223, 36224, 36225, and 36226.
So, if the doctor does an arch injection followed by selective internal carotid injection, you only bill 36223. Do not add 36221.
That is a common mistake that leads to denied claims.
Carotid Angiogram with Intervention: Adding 36227
What happens when the angiogram leads to a stent or balloon angioplasty?
You use 36227 for the selective internal carotid angiography when performed with an intervention.
Let me explain.
Code 36227 describes the diagnostic part of the procedure when the doctor already knows they are going to treat the vessel. It replaces 36223 in these scenarios.
But wait—you also have the intervention codes. For example:
-
37215 – Transcatheter placement of intravascular stent(s), cervical carotid artery, with distal embolic protection
-
37216 – Same as above, without embolic protection
-
37218 – Transcatheter placement of intravascular stent(s), intrathoracic common carotid or innominate artery
Here is the rule. You do not bill 36223 and 36227 together. You pick one.
-
Diagnostic only = 36223
-
Diagnostic leading to same-session intervention = 36227 plus the intervention code
But read the note carefully. If the doctor does a full diagnostic angiogram, then decides to intervene, you may report both the diagnostic and intervention codes with modifier 59. However, many payers consider the diagnostic portion as part of the intervention.
This is a gray area. The AMA says 36227 is for the diagnostic work when the intervention is planned. If the intervention was not planned, some coders use 36223 with modifier 59. Others use 36227 anyway.
When in doubt, follow your payer’s written policy.
Critical Documentation Requirements
You cannot pick the correct code without good documentation. That is not just a billing rule. It is patient care.
The doctor’s note must include:
-
Vessel name (right internal carotid, left common carotid, etc.)
-
Catheter type and size (e.g., 5-French diagnostic catheter)
-
Selective vs. non-selective wording
-
Contrast type and amount (if required by payer)
-
Projections taken (AP, lateral, oblique)
-
Findings (percent stenosis, plaque morphology)
-
Medical necessity (symptoms, prior imaging, planned surgery)
Missing any of these can sink your claim.
Here is a quick checklist for your file.
Documentation Checklist for Carotid Angiogram Coding
Was the catheter placement selective or non-selective?
Which specific artery was imaged?
Was an intervention performed in the same session?
Was the intervention planned before the angiogram?
Are there separate findings for each vessel imaged?
Does the medical necessity match the procedure?
If you answer “no” to any of these, go back to the provider.
Common Billing Scenarios and Correct Codes
Let us walk through real-world examples. These will help you see the code selection process in action.
Scenario 1: Routine Diagnostic Carotid Angiogram
The procedure: The doctor selectively catheterizes the right internal carotid artery. Three injections. Images show 40% stenosis. No intervention.
The correct code: 36223 (right internal carotid angiography)
Do not add: 36221 or 36222
Scenario 2: Bilateral Study for Pre-Surgical Planning
The procedure: The doctor selectively catheterizes the right common carotid, then the left common carotid. No internal carotid selection. The patient has a known carotid body tumor.
The correct code: 36222 with modifier 50 (bilateral common carotid angiography)
Or: 36222 (right) and 36222 (left) with modifier 59 on the second
Scenario 3: Arch Study Only
The procedure: The doctor places a pigtail catheter in the aortic arch. One injection. Images show patent great vessels. No selective catheterization.
The correct code: 36221 (non-selective arch angiography)
Do not add: Any selective code
Scenario 4: Diagnostic Angiogram Leading to Stent
The procedure: The doctor selectively catheterizes the left internal carotid. Finds 85% stenosis. Decides to place a stent with embolic protection.
The correct code: 36227 (diagnostic internal carotid with intervention) plus 37215 (stent with embolic protection)
Do not add: 36223
Scenario 5: Planned Intervention with Pre-Procedure Diagnostic
The procedure: The patient is scheduled for a carotid stent. The doctor does a limited diagnostic run to confirm anatomy, then places the stent.
The correct code: 36227 plus 37215
Reason: The diagnostic work is bundled into 36227.
Modifiers You Need to Know
Modifiers can save your claim or sink it. Use them carefully.
| Modifier | When to Use | Example |
|---|---|---|
| 50 | Bilateral procedure | Right and left internal carotid angiography |
| 59 | Distinct procedural service | Separate vessel not normally reported together |
| XS | Separate structure (more specific than 59) | Right external carotid after right internal carotid |
| 26 | Professional component | Reading the images (for facility-based providers) |
| TC | Technical component | Equipment and staff (for facilities) |
Most outpatient carotid angiograms are reported as a global service (professional and technical together). But if you work in a hospital setting, you may split the code.
Ask your billing manager which modifier your payer prefers for bilateral services.
Payer-Specific Policies You Cannot Ignore
Here is where many billers get into trouble.
Medicare and commercial insurers do not always agree on carotid angiogram coding.
-
Medicare – Follows NCCI edits strictly. Does not allow separate payment for diagnostic angiography before planned intervention. Requires modifier 50 for bilateral.
-
UnitedHealthcare – Requires documentation of medical necessity for each selective vessel. May deny 36223 if the patient had a CTA within 90 days.
-
Aetna – Considers diagnostic angiography part of the intervention. Do not bill 36223 with 37215 unless the diagnostic was truly separate and unexpected.
-
Cigna – Follows AMA guidelines closely. Accepts modifier 59 for separate vessel families.
Always check the specific policy. Do not assume one size fits all.
I will give you an example. A practice in Florida billed 36223 and 37215 for the same session. Medicare denied the 36223. The practice appealed and lost because the documentation did not prove the diagnostic study was medically necessary separate from the intervention.
That was a $900 mistake.
What About Imaging Guidance and Supervision?
Carotid angiography requires direct supervision by a qualified physician. That means the doctor must be in the room during the procedure.
For billing purposes, the professional component (modifier 26) covers:
-
Supervision of the procedure
-
Image interpretation
-
Written report
The technical component (modifier TC) covers:
-
Equipment
-
Technologist time
-
Supplies
-
Contrast media
In an office setting, you typically bill the global service (no modifier). In a hospital outpatient department, the hospital bills TC, and the physician bills 26.
Do not confuse this with the code for the angiogram itself. The CPT code stays the same. You just add the modifier.
How to Avoid the Most Common Denials
Denials for carotid angiogram codes usually fall into three buckets. Let us solve each one.
Denial 1: Bundling Issues
Problem: You billed 36221 and 36223 together.
Solution: Remove 36221. The selective code includes the non-selective work.
Denial 2: Missing Medical Necessity
Problem: The payer denied 36223 because the patient did not have symptoms or prior imaging showing the need.
Solution: Ask the provider to add a clear medical necessity statement. Examples include:
-
“Patient with transient right arm weakness and aphasia”
-
“Carotid duplex showing 70-80% stenosis”
-
“Pre-operative planning for carotid endarterectomy after positive CTA”
Denial 3: Incorrect Modifier for Bilateral
Problem: You billed two units of 36223 without a modifier. The payer paid one and denied the other.
Solution: Add modifier 50 to one unit of 36223. Or use modifier 59 on the second line item. Know your payer’s preference.
Important Notes for Readers
Note 1: Never report a selective carotid angiogram code without documentation of selective catheterization. A “power injection” through a non-selective catheter does not count.
Note 2: If the doctor images the internal carotid but the report says “catheter in the common carotid,” that is not selective. You need 36222, not 36223.
Note 3: Carotid angiogram codes are unilateral unless you use modifier 50 or 59. One code equals one vessel side.
Note 4: Always check the AMA CPT manual for the most current code descriptors. Codes change. Your reference book from three years ago is outdated.
Note 5: When in doubt, query the provider. A two-minute conversation can save a two-month appeal.
The Relationship Between Carotid Angiography and Other Imaging
Patients often have multiple imaging studies before an angiogram. You need to understand how this affects your code selection.
-
Carotid duplex ultrasound (CPT 93880) – Non-invasive. No contrast. Used for screening.
-
CTA of the neck (CPT 70498) – CT-based. Good for anatomy but less dynamic.
-
MRA of the neck (CPT 70547) – MR-based. No radiation but slower.
None of these replace the need for a diagnostic angiogram. But payers may require that the patient had one of these less-invasive tests first. If the doctor goes straight to angiography without a prior non-invasive test, the claim may deny for lack of medical necessity.
Document why the angiogram was necessary without prior imaging. Examples include:
-
“Patient too unstable for MRI”
-
“Prior CTA equivocal”
-
“Allergy to CT contrast requiring intra-arterial approach”
Frequently Asked Questions (FAQ)
1. What is the CPT code for a diagnostic carotid angiogram?
The most common code is 36223 for selective internal carotid angiography. But the correct code depends on which vessel the doctor catheterized.
2. Can I bill for both a carotid angiogram and a cerebral angiogram in the same session?
Yes, but you need separate documentation and a modifier like 59 or XS. The carotid codes (36222-36224) and cerebral codes (36226-36228) are distinct families.
3. Does Medicare cover carotid angiograms?
Yes, for medically necessary indications such as symptomatic carotid stenosis, prior TIA or stroke, or pre-procedural planning for endarterectomy or stenting.
4. What modifier do I use for bilateral carotid angiograms?
Use modifier 50 for one line item. Some payers accept two line items with modifier 59. Check your local MAC policy.
5. How do I code a carotid angiogram that turns into a stent?
Use 36227 (diagnostic with intervention) plus the stent code (37215 or 37216). Do not use 36223.
6. What is the difference between 36223 and 36227?
36223 is for diagnostic angiography alone. 36227 is for diagnostic angiography performed immediately before or during an interventional procedure on the same vessel.
7. Can a non-physician bill for carotid angiogram supervision?
No. Direct supervision by a qualified physician is required for the professional component (modifier 26).
8. How many carotid angiogram codes can I bill in one session?
You can bill multiple selective codes if the doctor documents separate, medically necessary catheterizations of distinct vessel families. But NCCI bundles many combinations. Always check the edits.
Final Thoughts on Getting Paid Correctly
Carotid angiogram coding is not just about picking a number from a list. It is about reading the documentation, understanding the anatomy, and knowing your payer’s rules.
The single best thing you can do is communicate with your providers. Show them this article. Ask them to use precise language like “selective catheterization of the right internal carotid artery” instead of “carotid angiogram.”
That small change can be the difference between a paid claim and a denial.
Keep this guide handy. Refer to it when you have a tricky case. And remember: when in doubt, query the provider.
Additional Resource
For the most current NCCI edits and Medicare Local Coverage Determinations (LCDs) for carotid angiography, visit the CMS Coverage Database:
https://www.cms.gov/medicare-coverage-database/indexes/national-and-local-indexes
Bookmark this link. Check it quarterly. Policies change.
Conclusion
Choosing the correct CPT code for a carotid angiogram requires attention to the vessel selected, the documentation provided, and the presence of any intervention. Code 36223 remains the standard for diagnostic internal carotid studies, while 36227 applies when an intervention follows. Always verify payer policies, use modifiers appropriately, and prioritize clear communication with your providers to ensure clean claims and proper reimbursement.
Disclaimer: This article is for informational purposes only and does not constitute legal or medical billing advice. CPT codes are copyright of the American Medical Association. Always verify payer-specific requirements.
Author: Medical Billing Team
Date: APRIL 03, 2026





