If you are navigating the world of spine surgery billing, you know that precision is everything. One small mistake can lead to denied claims or audits. Among the most common—yet confusing—procedures is the L5-S1 discectomy.
So, what is the exact CPT code for an L5-S1 discectomy? The honest answer is: it depends on the surgical approach and technique.
You cannot simply memorize one number. You need to understand the logic behind the code selection. This guide will walk you through the specific codes, the clinical documentation required, and the traps to avoid.
We will keep the language simple and clear. Whether you are a coder, a biller, or a surgeon trying to understand the process, this article is for you.
CPT Code for L5-S1 Discectomy
Understanding the L5-S1 Level
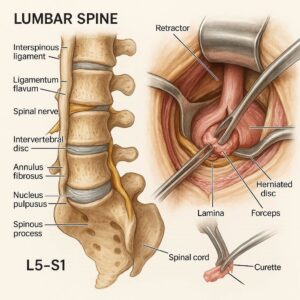
Before we jump into the numbers, let’s look at the anatomy. L5-S1 is the lumbosacral junction. It connects your lower spine to your sacrum. This area handles a lot of movement and weight.
Because of this stress, herniated discs at L5-S1 are very common. A discectomy here involves removing part of an intervertebral disc to relieve pressure on a nerve root.
Why does the level matter? Usually, it doesn’t change the base code. The code is typically the same for L3-L4, L4-L5, or L5-S1. What changes the code is how the surgeon gets to that disc.
Primary CPT Codes for L5-S1 Discectomy
Let’s cut to the chase. For a standard lumbar discectomy at L5-S1, you will likely use one of two main code families.
63030: The Workhorse Code
CPT 63030 is the most common code for this procedure. The official descriptor is: “Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar.”
In plain English, this means:
-
The surgeon makes a small opening in the bone (laminotomy).
-
They go in from one side (hemilaminectomy).
-
They remove the disc material pressing on the nerve.
-
This covers one level (like L5-S1).
Important Note: Code 63030 is for a unilateral approach. That means the surgeon works on only one side of the spine (left or right). If the patient has herniation on both sides? That is rare, but we will discuss that later.
63047: When You Need More Room
Sometimes, a simple laminotomy is not enough. If the patient has significant spinal stenosis (narrowing of the canal), the surgeon may need to remove more bone.
CPT 63047 is used for a laminectomy (complete removal of the lamina) rather than just a laminotomy. The descriptor includes decompression of nerve roots, but it implies a more extensive bone removal.
Here is the simple rule of thumb:
-
Use 63030 for a small, focused discectomy.
-
Use 63047 for a wide decompression plus discectomy.
Do not guess. Read the operative report. If the surgeon documents “bilateral decompression” or “extensive laminectomy,” 63047 might be your code.
Minimally Invasive Options (MIS)
Spine surgery has evolved. Many surgeons now perform L5-S1 discectomies using a microscope or an endoscope. Good news: The CPT code usually does not change.
CPT codes describe the work performed, not the technology used. If the surgeon uses a microscope to perform a hemilaminotomy and discectomy, you still report 63030.
However, there is an exception: Percutaneous endoscopic discectomy.
For this technique, you might look at Category III codes (temporary codes for emerging technology). Specifically:
-
0274T (Lumbar percutaneous discectomy)
-
0275T (with laminotomy)
Disclaimer: Category III codes are not universally reimbursed. Always check with the specific payer before using 0274T for an L5-S1 discectomy.
Comparison Table: 63030 vs. 63047 vs. 63056
To make this clearer, here is a simple comparison table.
| CPT Code | Procedure Name | Typical Use at L5-S1 | Bone Removal | Approach |
|---|---|---|---|---|
| 63030 | Lumbar discectomy (1 level) | Small, focal herniation | Partial (Laminotomy) | Unilateral |
| 63047 | Laminectomy with discectomy (1 level) | Herniation with stenosis | Complete (Laminectomy) | Usually bilateral |
| 63056 | Transpedicular approach | Recurrent herniation or complex pathology | Extreme lateral | Posterior/Transpedicular |
63056 is listed here for completeness. It is rare for a standard L5-S1 first-time discectomy. You will almost never use this unless the surgeon goes through the pedicle (the “foot” of the vertebra).
The “One Level” Rule
Let’s say the surgeon operates at L5-S1 only. That is one interspace. You bill one unit of service.
Do not accidentally bill for L4-L5 and L5-S1 if the surgeon only touched L5-S1. The code descriptor explicitly says “1 interspace.”
What if the surgeon does a discectomy at L4-L5 AND L5-S1 during the same surgery?
-
You would report 63030 for L4-L5.
-
You would report 63030-59 (Distinct procedural service) for L5-S1.
-
Or, better yet, use 63035 (each additional interspace) if the payer accepts it.
List of common add-on codes:
-
63035 (Add-on for each additional level of discectomy)
-
63048 (Add-on for each additional level of laminectomy with discectomy)
Do not forget the modifier. Without modifier 59 or XS (Separate structure), the payer will assume both codes are for the same level and deny one.
Modifiers You Need to Know
Modifiers are the second half of your coding equation. For an L5-S1 discectomy, keep these three in your pocket.
Modifier 50 (Bilateral Procedure)
Can you use 63030 with modifier 50? This is a gray area. A true bilateral discectomy at the same level (L5-S1 left and right) is extremely rare. Most payers expect you to bill 63030 once because the code already includes decompression of “nerve root(s)” (plural). Unless the surgeon documents separate incisions or distinct pathology on both sides, avoid modifier 50.
Modifier 59 (Distinct Procedural Service)
Use this when you have two different levels (e.g., L4-L5 and L5-S1) or when the surgeon does a discectomy plus an unrelated procedure at the same level (e.g., a bone biopsy). In 2026, consider using the more specific XS (Separate structure) or XP (Separate practitioner) modifiers instead of 59.
Modifier 22 (Increased Procedural Services)
The surgery took twice as long due to scar tissue or obesity? You might add modifier 22. You will need to send the operative report and a cover letter explaining why. Do not abuse this. Only use it for true outliers.
What About the Surgical Approach? (Anterior vs. Posterior)
An L5-S1 discectomy is almost always done from the posterior (back) or posterolateral (from the back and side).
You will rarely, if ever, see an anterior (through the belly) discectomy at L5-S1. That approach is more common for artificial disc replacement or fusion.
If a surgeon claims to do an anterior discectomy at L5-S1 for a simple herniation, verify the documentation. The code would likely be 22558 (Anterior lumbar interbody fusion), not a simple discectomy code.
Stick to the posterior codes (63030, 63047) for 99% of L5-S1 discectomies.
Recurrent Disc Herniation at L5-S1
What happens when the disc herniates again at the same level, L5-S1? The patient had a discectomy six months ago, and now the pain is back.
The code changes.
For a recurrent disc herniation, the standard codes (63030) are often incorrect. The surgeon has to cut through scar tissue. This is more difficult and time-consuming.
Look at:
-
63030 with modifier 22 (if the payer does not have a specific code).
-
63042 (Laminotomy for recurrent herniation – this is the preferred code if available for your payer).
Some coders argue that 63042 is for a redo laminotomy. However, many payers still expect 63030 with extensive documentation. Check your local coverage determination (LCD).
“The hardest part of coding a redo L5-S1 discectomy is proving the medical necessity. The operative report must explicitly state ‘recurrent herniation at the same level’ and describe the dissection of scar tissue.” — Senior Spine Coder, 2026
Bundling Rules: What Not to Bill Separately
This is where new coders lose money or get audited. Certain services are bundled into the discectomy code. You cannot bill them separately.
Do not separately bill the following with 63030 or 63047:
-
Laminotomy (It is part of the code).
-
Foraminotomy (Part of the code).
-
Flavectomy (Removal of ligamentum flavum – it is included).
-
Exploration of nerve root (Included).
-
Microscope use (Included in the surgical code unless your payer allows S2900 – rare).
You can bill separately for:
-
Fluoroscopy (Guidance with X-ray) – Use 77002 (fluoroscopic guidance for needle placement) or 77003 (for catheter/injection) if documented. Many payers bundle this now, so check your fee schedule.
-
Intraoperative monitoring (IOM) – Use 95940 (continuous intraoperative monitoring) if a separate provider (not the surgeon) performs it.
Real-World Examples
Let us walk through three patient scenarios. This will help you apply the theory.
Scenario 1: The Simple Case
Patient: John, 35 years old.
MRI: Left-sided L5-S1 disc herniation.
Surgery: Left paramedian incision. Left L5 hemilaminotomy. Excision of herniated disc fragment at L5-S1. Nerve root decompressed.
CPT Code: 63030 (One level, unilateral, lumbar).
Modifier: None.
Scenario 2: The Stenosis Case
Patient: Maria, 68 years old.
MRI: L5-S1 central disc herniation with severe spinal stenosis.
Surgery: Midline incision. Complete L5 laminectomy. Bilateral decompression. Removal of disc material at L5-S1.
CPT Code: 63047 (Laminectomy with discectomy – the bone removal is extensive).
Modifier: None.
Scenario 3: The Two-Level Case
Patient: Robert, 48 years old.
MRI: Herniated discs at L4-L5 (right side) and L5-S1 (left side).
Surgery: Surgeon performs right L4-L5 discectomy (63030). Then performs left L5-S1 discectomy (63030).
CPT Code: 63030 (for L4-L5) and 63030-59 (for L5-S1).
Alternative: Some coders use 63035 for the second level. Check payer preference. In 2026, many prefer 63030 with XS modifier.
Common Billing Mistakes for L5-S1 Discectomy
Let us list the most frequent errors. Avoid these to keep your claims clean.
-
Mistake #1: Using 63030 for a bilateral laminectomy. If the surgeon took the whole lamina, use 63047.
-
Mistake #2: Forgetting the operative report must say “L5-S1.” If it says “lumbosacral junction,” that is fine. But if it says “lower lumbar,” ask for clarification.
-
Mistake #3: Billing for a fusion when only a discectomy was done. Check the title of the procedure. “Discectomy only” vs. “Discectomy with fusion” (which would use 22558 or 22630).
-
Mistake #4: Using the unlisted code 64999. Do not do this unless there is literally no other code. 63030 exists for a reason.
Documentation Requirements for Surgeons
As a surgeon, you can help your coder by including five specific details in your op report for an L5-S1 discectomy.
-
Level: Explicitly write “L5-S1.” Do not write “L5-S1 interspace”?
-
Side: Write “Left,” “Right,” or “Bilateral.”
-
Technique: Write “Hemilaminotomy” (partial) or “Laminectomy” (complete).
-
What was removed: “Herniated disc fragment” or “Annular tissue.”
-
Decompression: “Nerve root was visualized and free.”
Without these five elements, the coder is guessing. And guessing leads to denials.
How Payers View L5-S1 Discectomy Codes in 2026
Reimbursement for spine surgery is tightening. Commercial payers and Medicare are using AI to audit notes.
They look for:
-
Medical necessity: Does the MRI match the operative level? If the MRI shows L4-L5 herniation but the surgeon operated on L5-S1, the claim will deny.
-
Modifier usage: Overuse of modifier 22 will trigger a review.
-
Frequency: One 63030 per patient per year is normal. Two in six months for the same level is a red flag (unless it is a recurrence).
Always check your local MAC (Medicare Administrative Contractor) for their specific LCD on lumbar discectomy.
CPT Codes for Related Procedures at L5-S1
Sometimes, a discectomy is part of a bigger surgery. Here is a quick look at related codes.
| Procedure | CPT Code(s) | Notes |
|---|---|---|
| L5-S1 Discectomy with Fusion (Posterior) | 22630 (fusion) + 63030 or 63047 | Do not bill 63047 and 22630 together? Some payers bundle. Use 22630 alone if the code includes decompression. |
| L5-S1 Discectomy with Artificial Disc | 22857 (Total disc arthroplasty) | This includes the discectomy. Do not bill 63030 separately. |
| L5-S1 Revision Discectomy | 63042 or 63030-22 | Requires strong documentation. |
| Epidural Injection after surgery | 62323 | Only if done at a different session. Not on the same day. |
FAQ: CPT Code for L5-S1 Discectomy
Q1: Is there a specific CPT code just for “L5-S1” level?
No. CPT codes do not specify vertebral levels. The level (L5-S1) must be documented in the operative report, but the code (e.g., 63030) is the same for any lumbar level.
Q2: Can I use 63030 for an L5-S1 microdiscectomy?
Yes. “Micro” refers to the use of a microscope. There is no separate code for microdiscectomy. 63030 is the correct code.
Q3: What is the difference between 63030 and 63020?
63020 is for the cervical spine (neck). 63030 is for the lumbar spine (low back). Do not confuse them. L5-S1 is lumbar, so use 63030.
Q4: How do I bill for an L5-S1 discectomy performed through a tubular retractor?
Use 63030. The approach (open vs. tubular vs. endoscopic) does not change the base code unless you use a percutaneous technique (0274T).
Q5: What if the surgeon only removes the disc without any bone removal?
That is rare. A true “discectomy without laminotomy” is almost impossible because the disc is behind the bone. However, for a far-lateral herniation, the surgeon might go outside the bone. In that case, 63055 (Transpedicular or extrapedicular approach) might apply. For 99% of L5-S1 cases, stick to 63030.
Q6: What modifier do I use for L5-S1 discectomy on the left and right sides?
If the surgeon does a true bilateral decompression at L5-S1, use 63047 (which typically implies bilateral). If using 63030, append modifier 50. However, many payers prefer 63047 for bilateral work.
Q7: Is 63030 globally packaged?
Yes. 63030 includes the pre-op visit (day of surgery), the surgery itself, and 90 days of post-op care. Do not bill separate E/M codes for routine follow-ups.
Additional Resource for Spine Coders
For the most up-to-date information on lumbar spine coding, visit the American Academy of Professional Coders (AAPC) website. Their spine coding forum is an excellent resource for real-world advice on L5-S1 discectomy denials and appeals.
👉 Recommended Link: www.aapc.com/discussions/forum/spine-coding
Note: Always verify codes with your current CPT manual and payer policies, as codes and guidelines change annually.
Important Note for Readers
Disclaimer: This article provides general guidance for educational purposes. Medical coding is complex and payer-specific. CPT codes are copyright of the American Medical Association. Always verify codes using the current CPT manual and your specific payer’s medical policy. The author and publisher are not liable for claim denials or audit penalties resulting from the use of this information. When in doubt, consult a certified professional coder (CPC).
Conclusion
Let us wrap this up in three simple lines.
First, the standard CPT code for a unilateral L5-S1 discectomy is 63030. Second, if the surgeon performs a complete laminectomy (extensive bone removal), use 63047 instead. Third, always document the specific level (L5-S1), side, and approach in the operative report to avoid denials and audits.





