If you work in interventional radiology, medical coding, or billing, you know that Y90 radioembolization—often referred to as Selective Internal Radiation Therapy (SIRT)—is a life-saving procedure for patients with primary and metastatic liver cancer.
However, capturing the correct reimbursement for this complex, multi-step procedure can feel like navigating a maze. You aren’t just billing for one “shot.” You are billing for a sophisticated process involving mapping, planning, and the therapeutic delivery itself.
In this guide, we will demystify the CPT code for Y90 radioembolization. We will break down exactly which codes apply, how to avoid common denial pitfalls, and how to structure your claims for success.
CPT Codes for Y90 Radioembolization
Understanding the Complexity of Y90 Radioembolization
Before we dive into the numbers, it is crucial to understand why coding this procedure is different from a standard injection.
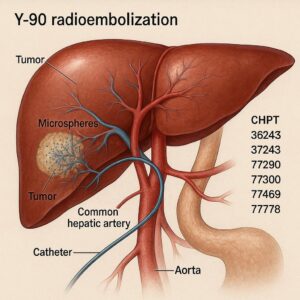
Yttrium-90 (Y90) radioembolization is a form of brachytherapy. Tiny glass or resin microspheres loaded with radioactive Y90 are infused into the hepatic artery. These spheres lodge in the tumor’s microvasculature and deliver high doses of radiation directly to the cancer cells.
Because it involves radiation oncology and interventional radiology, the coding structure typically splits into two distinct parts:
-
The Mapping/Angiography (Planning)
-
The Delivery (Therapeutic infusion)
The Primary CPT Codes for Y90
When billing for Y90 radioembolization, you will generally use a combination of codes from the Surgery/Radiology sections of the CPT manual.
The Delivery Code: 79445
The primary code for the therapeutic delivery of Y90 is CPT 79445.
-
Official Descriptor: *Radiopharmaceutical therapy, by intra-arterial particulate administration (e.g., yttrium-90)*
-
When to use it: This code represents the actual infusion of the Y90 microspheres. It includes the administration of the radioactive material, the patient preparation for radiation therapy, and the technical supervision of the infusion.
-
Key Note: This is a “global” code in the sense that it covers the therapeutic dose administration. However, it does not cover the vascular access or mapping performed on a different day.
The Mapping and Planning Codes: 37242 & 37243
Before the actual treatment can happen, the interventional radiologist must perform a visceral angiography to map the liver vasculature. This is often done 1–2 weeks prior to the treatment. The goal is to identify the arteries feeding the tumor and to prophylactically embolize (block) vessels that lead to the stomach or bowel to prevent radiation injury.
There are two primary codes for the mapping procedure, and choosing the correct one depends on what was done during the planning session:
-
CPT 37242: Transcatheter arterial embolization or occlusion, initial, for tumors, organ ischemia, or infarction; without *release of a radioactive element (e.g., yttrium-90)*
-
Use this: When the physician performs the mapping angiogram and embolizes (coils or particles) the non-target vessels (like the gastroduodenal artery) to protect the gut. This is the most common scenario for Y90 planning.
-
-
CPT 37243: Transcatheter arterial embolization or occlusion, initial, for tumors, organ ischemia, or infarction; with *release of a radioactive element (e.g., yttrium-90)*
-
Use this: If the physician performs the mapping and then proceeds to deliver a “test dose” of MAA (macroaggregated albumin) or if they deliver the Y90 on the same day as the mapping. However, in standard clinical practice, the mapping and delivery are separated by a lung shunt fraction study, making 37242 the more frequent choice for the planning day.
-
The Microsphere Selection: S2095
While not a CPT code (it is a HCPCS Level II code), S2095 is often billed by outpatient hospitals or some payers to distinguish the type of microsphere used.
-
Descriptor: *Transcatheter occlusion or embolization for tumor destruction, percutaneous, any method, using yttrium-90 microspheres (e.g., TheraSphere, SIR-Spheres)*
-
Note: Private payers and Medicare may handle this differently. Some prefer CPT 79445, while others want to see the S-code for the supply component. Always verify with your local MAC (Medicare Administrative Contractor).
Comparative Table: Mapping vs. Delivery
To visualize the workflow, here is how a standard Y90 case usually breaks down across two separate encounters.
| Procedure Stage | Typical CPT/HCPCS | Purpose | Key Inclusions |
|---|---|---|---|
| Stage 1: Mapping & Prophylaxis | 37242 | Angiography, vessel selection, and coiling of non-target vessels (GDA, right gastric). | Catheter placement, contrast injections, embolization coils, closure device. |
| Stage 1: Lung Shunt Study | 78800 or 78801 (nuclear medicine) | To calculate how much radiation may leak to the lungs. | Radiopharmaceutical injection (MAA) and imaging. |
| Stage 2: Therapeutic Delivery | 79445 | Infusion of Y90 microspheres into the tumor-feeding vessels. | Catheter placement, radiation safety protocols, dose calculation, infusion. |
| Stage 2: Device/Sphere | S2095 or C-code | The supply cost of the actual microspheres. | TheraSphere (glass) or SIR-Spheres (resin). |
Physician Billing vs. Hospital Outpatient Billing
One of the biggest sources of confusion in Y90 coding is the difference between how a physician (professional component) bills versus how a hospital (technical/facility) bills.
For the Physician (Professional Services)
The physician typically bills:
-
Mapping Day: 37242 (or 37243). This covers the professional work of the angiography, the decision making, and the embolization of non-target vessels.
-
Delivery Day: 79445. This covers the professional work of the Y90 infusion.
-
Modifiers: If the same physician performs the mapping and the delivery on separate days, no modifier is usually needed. If a different physician performs the delivery, you may use modifier -77 (Repeat procedure by another physician).
-
For the Hospital Outpatient Department (Facility)
Hospitals bill for the resources, supplies, and nursing staff. Their coding is more granular:
-
Mapping Day: 37242 (for the procedure room) plus CPT 75894 (if they use the old brachytherapy angiography code, though 37242 is currently preferred for facility billing as well). They also bill for coils (C1769) and contrast (A4642).
-
Delivery Day:
-
CPT 79445 (for the infusion suite/OR time)
-
S2095 or C-code (C2616 or C2637 depending on the sphere type) to capture the high cost of the Y90 spheres.
-
C1757 (Catheter, transluminal angioplasty, non-laser) if a specific microcatheter was used.
-
Important Note: Medicare and commercial payers are very strict about “bundling.” You cannot bill for a full angiography code (e.g., 75726) on the same day as 37242 or 79445 for the same vessel territory, as the angiography is considered integral to the embolization/therapy codes.
Modifiers: The Key to Avoiding Denials
Using the correct modifiers is just as important as using the correct codes. In Y90 radioembolization, you will frequently use:
-
Modifier -59 (Distinct Procedural Service): This is the most critical modifier. Because mapping (37242) and delivery (79445) are performed on different days, you generally do not need modifier -59. However, if the delivery is performed on the same day as a repeat mapping (rare), you would use -59 to show they are separate and distinct procedures.
-
Modifier -26 (Professional Component): When a physician bills for a procedure performed in a hospital setting, they append -26 to indicate they are billing only for their professional interpretation and work.
-
Example: A radiologist billing for the lung shunt study would use 78801-26.
-
-
Modifier -TC (Technical Component): Used by facilities or billing entities that own the equipment to bill for the technical portion of a service. Most hospitals bill globally (no modifier) for procedures, but if a mobile lab provides the equipment, they may use -TC.
Common Coding Pitfalls and How to Avoid Them
Even experienced coders can stumble on Y90 cases. Here are the three most common mistakes we see:
1. Billing for the Wrong Embolization Code
If the physician performed the mapping and did not place coils to protect the gut, 37242 might be incorrect. However, in the standard of care for Y90, prophylactic embolization is almost always required. If the doctor only performed a diagnostic angiogram and no embolization, you cannot bill 37242. You would have to revert to a standard angiography code (like 75726) for the mapping day.
2. Forgetting the Lung Shunt Study
The lung shunt study (LSS) is a critical step to ensure patient safety. This is a nuclear medicine procedure and is billed separately from the interventional radiology mapping.
-
Codes: 78800 (Radiopharmaceutical localization, vascular flow, single study) or 78801 (multiple studies). If the hospital uses a hybrid procedure suite, ensure the LSS is not accidentally bundled into the interventional radiology claim.
3. Same-Day Mapping and Delivery
Sometimes, a patient is deemed an “easy anatomy” case, and the physician performs the mapping and the Y90 infusion on the same day.
-
The Rule: If this happens, you cannot bill 37242 and 79445 together without a modifier to indicate they are separate and distinct (Modifier -59). However, payer policies vary widely.
-
Alternative: Some payers prefer that you bill 37243 (Embolization with release of radioactive element) for the combined session, rather than two separate codes. You must check your specific payer’s LCD (Local Coverage Determination).
A Step-by-Step Guide to Building Your Claim
Let’s walk through a typical patient scenario to see how the coding comes together.
Scenario: A 62-year-old patient with colorectal metastasis to the liver.
-
Day 1: Patient comes to Interventional Radiology. The physician performs a celiac and superior mesenteric artery angiogram. They identify a patent gastroduodenal artery (GDA) and embolize it using coils. They then place a catheter in the proper hepatic artery and inject MAA for a lung shunt study. The patient goes to Nuclear Medicine for imaging.
-
Day 14: Patient returns. The physician performs angiography to confirm vessel anatomy (no new intervention needed). They infuse Y90 TheraSpheres into the right and left hepatic arteries.
Physician Claim (Professional):
-
Day 1: 37242 (Transcatheter arterial embolization… without release of radioactive element)
-
Day 1 (Nuclear Med): 78801-26 (Radiopharmaceutical localization, multiple studies)
-
Day 14: 79445 (Radiopharmaceutical therapy, by intra-arterial particulate administration)
Hospital Outpatient Claim (Facility):
-
Day 1:
-
37242 (Facility resource)
-
C1769 (Guide wire/coils)
-
A4642 (Contrast material)
-
78801 (Nuclear medicine technical component)
-
-
Day 14:
-
79445 (Facility resource)
-
C2637 (TheraSphere Yttrium-90 microspheres)
-
C1757 (Catheter, micro)
-
The Importance of Documentation
No amount of coding expertise can save a claim if the physician’s documentation is lacking. For Y90 radioembolization, ensure the medical record clearly states:
-
Medical Necessity: Diagnosis codes (e.g., C78.7 for secondary liver cancer, C22.9 for primary liver cancer) must justify the procedure.
-
Vessel Selection: A clear description of which vessels were targeted and which were embolized.
-
Shunt Fraction: Documentation of the lung shunt fraction percentage and why it is safe to proceed.
-
Sphere Type: Documentation of whether glass (TheraSphere) or resin (SIR-Spheres) was used, as this impacts the HCPCS code for the supply.
Conclusion
Coding for Y90 radioembolization is a multi-faceted process that requires a strong understanding of interventional radiology and nuclear medicine principles. The primary CPT code for Y90 radioembolization delivery is 79445, but this is only the final piece of the puzzle. Success in reimbursement relies on accurately coding the mapping session with 37242, correctly appending modifiers for professional components, and meticulously capturing the supply costs for the microspheres.
By understanding the distinct phases of this therapy—planning and treatment—and adhering to the bundling rules of Medicare, you can ensure that your claims accurately reflect the complexity and value of this life-saving procedure.
Frequently Asked Questions (FAQ)
Q1: Can I bill CPT 79445 and CPT 37242 on the same day?
Generally, no. These represent two distinct phases of treatment that are typically performed on different days. If they are performed on the same day due to unique circumstances, you must append Modifier -59 to the secondary code and be prepared to provide documentation proving the services were separate and distinct. Most payers, however, expect the mapping and treatment to be separate encounters.
Q2: What is the difference between CPT 37242 and CPT 37243 for Y90?
The difference lies in the “release of a radioactive element.” 37242 is used when you are performing a mapping and embolization without giving the therapeutic dose (standard planning day). 37243 is used when the radioactive Y90 spheres are actually infused during that same session. Since most Y90 treatments are split across two days, 37242 is more common for the initial visit.
Q3: Is the lung shunt study included in the Y90 infusion code?
No. The lung shunt study (LSS) is a separate nuclear medicine procedure. It is not bundled into 79445 or 37242. You must bill the appropriate nuclear medicine code (78800, 78801, or 78807) for both the professional and technical components separately.
Q4: Does Medicare cover Y90 radioembolization?
Yes, Medicare covers Y90 radioembolization (SIRT) for primary and metastatic liver tumors, provided the patient meets specific medical necessity criteria outlined in Local Coverage Determinations (LCDs). Coverage often requires that the patient is not a candidate for surgical resection or ablation.
Q5: What diagnosis codes should I use?
The most common diagnosis codes are:
-
C22.9 – Malignant neoplasm of liver, not specified as primary or secondary.
-
C78.7 – Secondary malignant neoplasm of liver (for metastases).
-
C22.0 – Liver cell carcinoma (Hepatocellular carcinoma).
Always ensure the diagnosis supports the medical necessity for the procedure.
Additional Resources
For further reading and to stay updated on the latest coding changes, we recommend the following trusted resources:
-
The Society of Interventional Radiology (SIR) Coding Corner: SIR offers quarterly coding advice and webinars specifically focused on IR procedures like Y90.
-
CMS Local Coverage Determinations (LCDs): Search for “Yttrium-90 Microspheres” or “Y90” in the Medicare Coverage Database for your specific state to view local billing requirements.
Disclaimer: This article is intended for educational and informational purposes only. Medical coding guidelines are subject to change. It is the responsibility of the provider and coding staff to verify all codes with current payer policies and the latest AMA CPT manual. This does not constitute legal or medical advice.
Author: Professional Medical Coding Specialist
Date: April 01, 2026





